You may not be familiar with the term “coaching footprint” but perhaps you are more familiar with the term “carbon footprint”. One’s carbon footprint is defined as the amount of carbon dioxide released into the atmosphere as a result of the activities of a particular individual, organization, or community. The implication is that the way in which you choose to live comes with a trade-off. That trade-off may or may not be important to you, depending on what other concerns you have in your life, and whether or not the environment is something you think and care about.
The term “therapeutic footprint” was first used in 2006 by Anderson and colleagues. They described a model to plot the relationship between level of evidence and risk, and to analyse how that relationship varied in medical, complementary and alternative therapies.
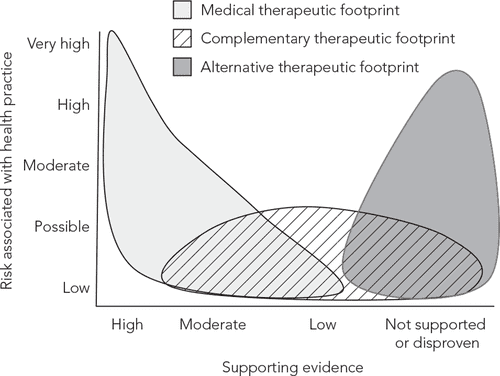
I recently saw the term used on Twitter by Sigurd Mikkelsen in a slightly different manner. It got me thinking about how this might apply beyond strictly healthcare, and how we might want to think about the “therapeutic footprint” concept in coaching / personal training (one-to-one, group, online etc.).

What Have I Left Behind?
When I (Gary) coach someone, I try to be conservative. I try my best to recognise that I am guiding someone on how they live their life. Whether it’s a change in the amount of time they allocate to exercise per week, the foods they buy, their pre-bed routine etc., it’s a change in the way that they live. I take that seriously. However, it’s clearly not just “what they do”, but also “why” they do the things they do, and also their attitudes, beliefs, knowledge, and so on. Even if I tell someone to do all of the right things, do I want them to be doing them for the wrong reasons? Do they now have more negative attitudes towards something? Are those attitudes justified? What have I left behind?
That’s the important part – what I leave behind. I consider this to be my Coaching Footprint. I care about it more than the % strength gained, weight lost, or kilometres ran. I believe that personal training, even in an online capacity, can be a very valuable part of our “frontline” healthcare system. But, that will only be the case if we treat ourselves as professionals. One of the central principles of healthcare is “first, do no harm”. I believe that we should carry that into the fitness profession(s).
First, Do No Harm
“Harm” in the fitness industry is acknowledged. This harm is generally exclusive to acute injury or illness. You will often see coaches and trainers virtue signal about how their clients are so healthy, injury free, never sick, not hungry etc. However, I would argue that a lot of the harm left behind, or, one’s coaching footprint, actually goes unnoticed. It is the fear of certain movements; of food; of weight gain; of living “impure”. It is the belief that for one to be healthy, one must reduce all life decisions to “positive” or “negative” for health. It is the attitude that health can be viewed through a purely biomedical lens, at the expense of one’s career, relationships, and sense of fulfillment. It is a flawed understanding of the principles of nutrition. It is the misapplication of “feelings” in exercise prescription. It is the debt incurred by one’s monthly supplement bill. It is the fear of not being “perfect”.
I wish I understood this sooner. Why? Well, I once had a much larger coaching footprint. I was not precise with my speech, nor was I considerate of the repercussions of the narrative delivered. If I thought something might have a chance of helping someone, I was all for it. I thought I was doing a better job by trying to have someone improve everything, rather than improving the things that had the greatest effect size. I would give advice, without considering potential misinterpretations or extrapolations either now, or in the future.
What Now?

I try to be conservative. When making decisions as to what advice I am going to give to someone, or how I might deliver it, I consider some of the following:
Cost – Is there any cost to the advice that I am about to give? If so, is it likely that this is within someone’s budget? If so, is this the most cost-effective way for this person to move closer toward the goals that they have set for themselves?
Example: If someone is going to invest in a supplement for “general health”, it would be fair for that person to assume that, based on what I have said, this supplement is a requirement for long term health. If this costs €40/mo, that is a cost of €480/yr. That is a lot, and hence, I should probably have a pretty strong justification.
Time – How much time is going to be invested by the person if I give them this advice? If so, is it likely that the person has this much time available? If so, is this the most time-efficient way for this person to move closer toward the goals they have set for themselves?
Example: If someone starts a “stretching routine” [in addition to resistance training] that is to be performed for 30 minutes daily, that is an investment of 3.5 hrs/wk, 14 hrs/mo, or 182 hrs/yr. That is a lot of time, and hence, I would want to know that this is really in line with that person’s goal (e.g. get better at stretching vs reduce injury risk, great for the former, not for the latter).
Attitudes/Beliefs – How might my advice modify someone’s attitudes/beliefs? Is my advice aligned with a specific narrative, and if so, is that a helpful one? How might this affect the way that someone views their health and fitness behaviours, and the other areas of their life?
Example: If I tell someone that they need to do specific exercises for their posture, one would assume that this aligns with the general narrative relating to posture and pain. This has the potential to reinforce preconceived notions about slouching and back pain, rounded shoulders being harmful etc.. Therefore, I must consider 1) the utility of the advice, and 2) the narrative that runs with it.
Justification – This is a simpler one, but is the information I am providing correct/true? And, how do I know? Is there a very high level of evidence (e.g. systematic reviews/meta-analyses on x intervention in populations similar to my client), or is this simply my opinion? If the justification is weak, then all of the previous questions become even more important. If advice is based on weak, unsubstantiated claims, is also part of an unhelpful narrative, and carries a significant cost and time investment, then that’s probably not great advice.
Example: If I tell someone they need to follow a specific meal plan with specific foods, requiring someone to eat every 3 hours to lose body fat, that’s 1) not justified based on the evidence, 2) potentially harmful to one’s attitudes/beliefs toward nutrition, and 3) a large investment of time (meal prep, specific shopping) and potentially money.
A Framework for Assessing Your Coaching Footprint
While we have been discussing the concept of your coaching footprint and framing it specifically as “what am I leaving behind?”, it can actually be quite difficult to contextualise this and assess your coaching footprint. So, we wanted to actually share some concrete examples. Before we get there, I would like you to understand what we are really suggesting that you consider when thinking about your coaching footprint.
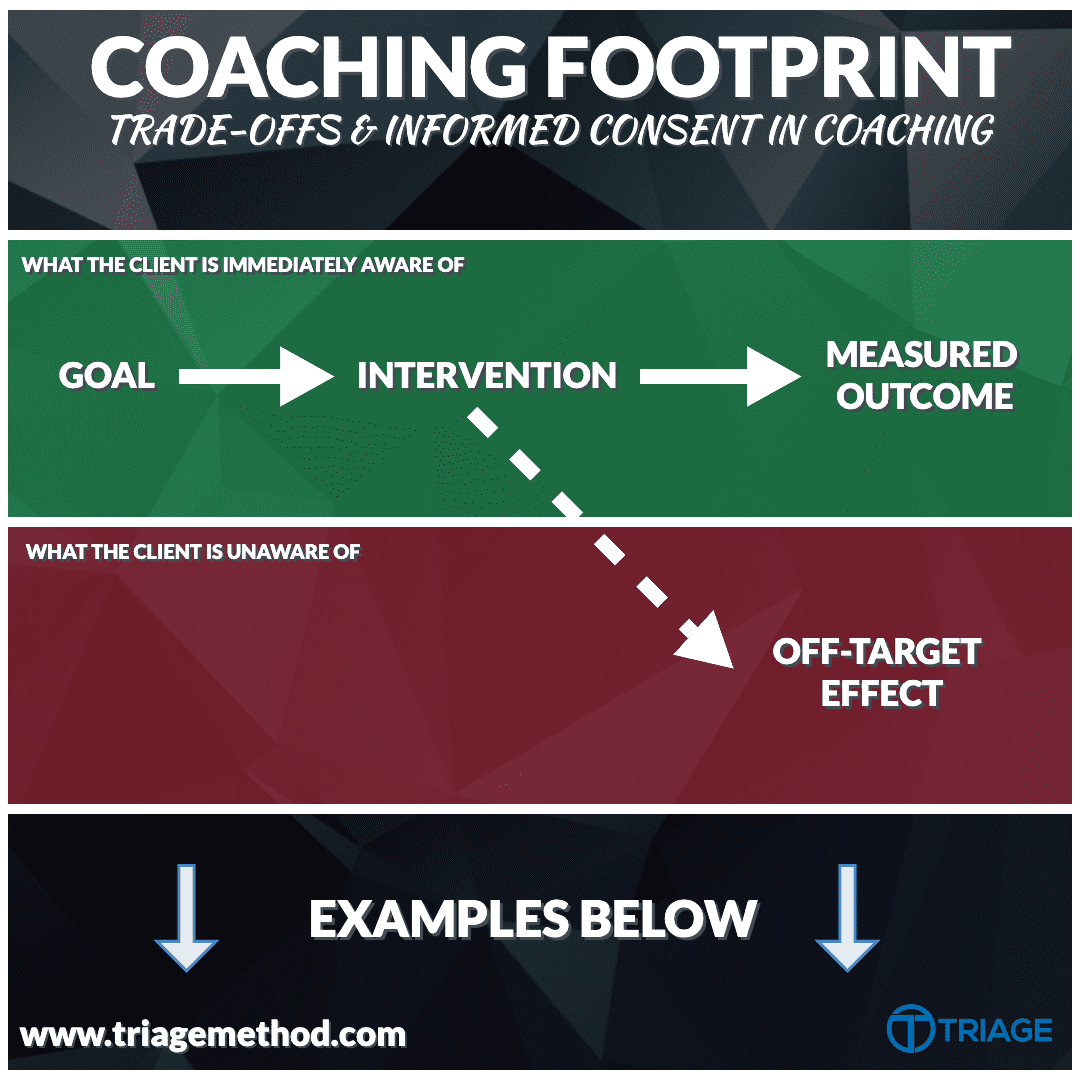
Every client that signs up with a coach will have some sort of goal that they are hoping to achieve. They may not be clear on exactly what that goal is. In some cases, it’s an objective outcome for a specific purpose, such as breaking a record in sport. In others, it’s some sort of feeling. A feeling of self-worth, of satisfaction with one’s body, of pride in one’s capacity for movement, strength, muscularity, etc. This is something most coaches are aware of, but the trade-offs that the client is willing to accept often go undiscussed. Sometimes, this is because the client themselves may not realise what the trade-offs are and the coach assumes that they do, but oftentimes, the coach themselves may not even be aware of the trade-offs, or they may simply not understand the extent to which these trade-offs could affect the individual’s quality of life.
Therefore, what we propose in this article is that, when you make a coaching decision, you don’t simply ask “what is the intervention that will lead to the desired outcome?”, but also “what are the trade-offs or off-target effects to which I or my client may currently be blind?”. By doing this, you can ensure that your interventions are appropriately selected and that you are adhering to the process of informed consent in your coaching practice.
Psychosocial Example
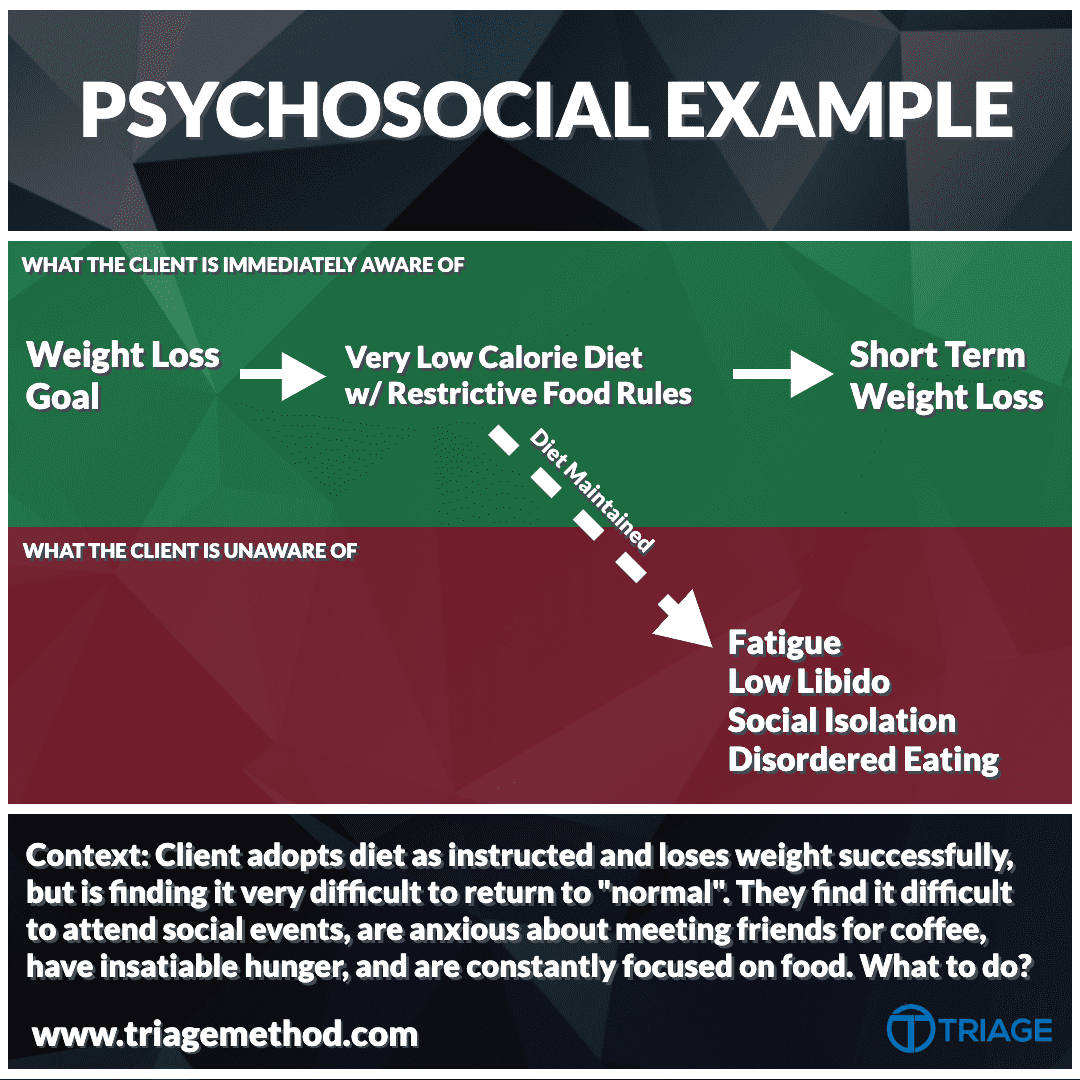
In this first example, you will notice a very common occurrence in dieters pursuing fat loss, especially if embarking on a very restrictive diet with limited food choices. If you adhere to a 1000 calorie diet that is permissive of no more than lean meats and vegetables, will you lose weight? Absolutely. But, whether or not this is appropriate for a given individual depends on additional context.
For an individual with Type 2 Diabetes hoping to put the disease into remission, a very low-calorie diet may actually be a great call that is absolutely worth the trade-off of restricted food choices (Taylor 2019). But, for a client with a history of yo-yo dieting and psychological risk factors for the development of disordered eating, this may be a poor option (Linardan 2019).
Therefore, considering the trade-offs of the intervention for the individual seeking your coaching is a key component in assessing your coaching footprint. The coaching footprint for a given intervention is not fixed, but rather will vary within in and between individuals over time.
Weight Loss Diet Example
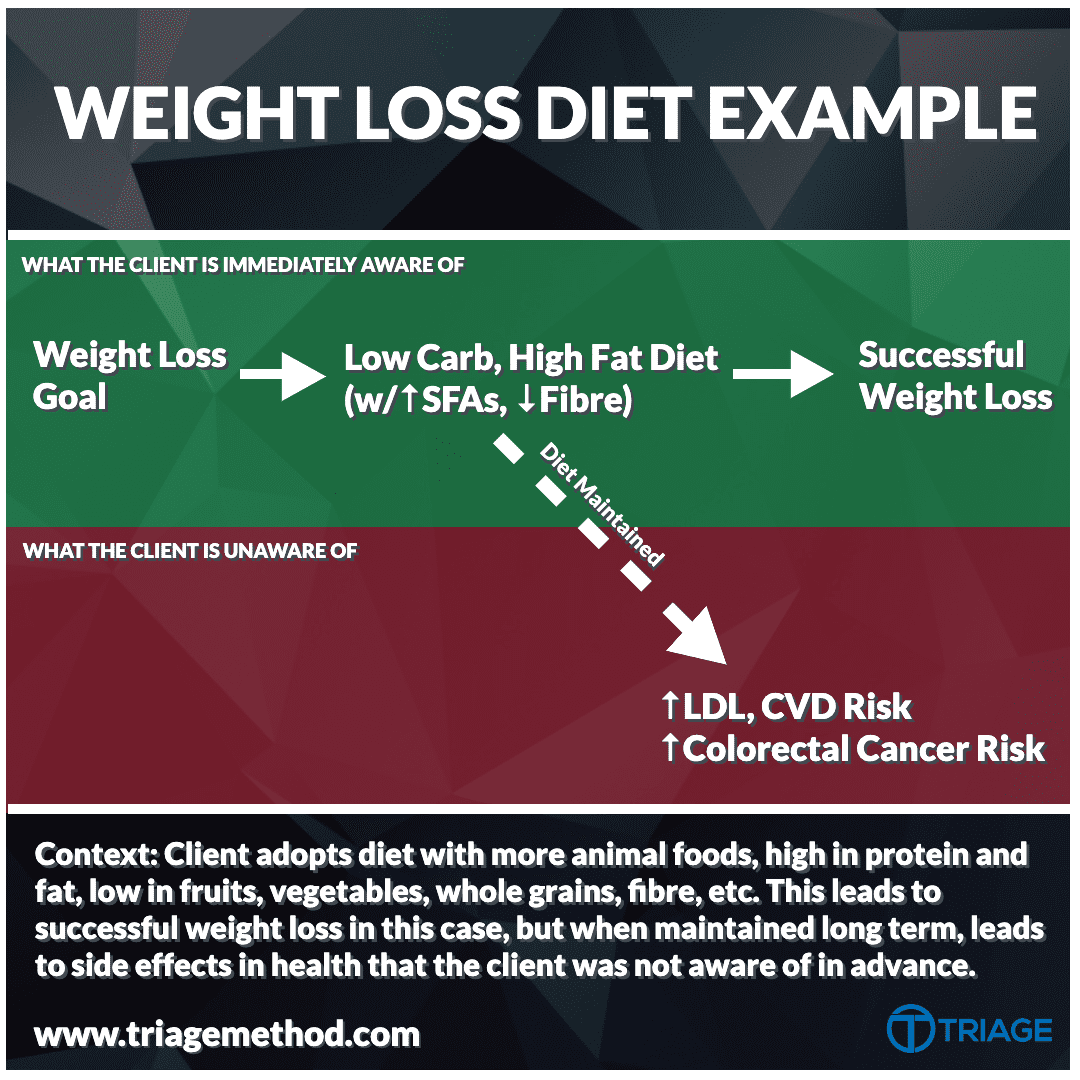
In this example, we are looking at a successful weight loss outcome. If we were to analyse weight loss in isolation, we would consider this a win. As a coach, you could share your transformation photos on-site and be happy that you did a great job. But, what about the effects of your chosen dietary intervention on the individual’s long-term health?
In this case, let’s assume the coach adheres to claims made by low-carb high-fat (LCHF) diet proponents that saturated fat doesn’t matter, cholesterol and heart disease is all a lie, and how much meat you eat just doesn’t matter. It is likely that, in this context, the client may see an increase in their LDL cholesterol over time (Retterstøl et al. 2018). Even though they may have improved their health through weight loss, their cardiovascular risk would be increased as a result of this increase in LDL cholesterol; this does not mean their health has worsened overall, but rather that there may be an excess risk that could have been avoided while achieving similar health outcomes in other domains (e.g. if excess saturated fat had been swapped for unsaturated sources) (Bóren et al. 2020).
Weight Gain Diet Example

In this example, we are really looking at the long-term effects of persistent weight gain, especially in the context of a diet that has been adopted due to the ease with which it leads to overfeeding. Often, when people are struggling to gain muscle, they will adjust their diet in favour of foods that are easier to overconsume, which can include eating foods that are effectively a mix of salt, refined carbohydrates and/or sugar, and fat. In the short term, this probably isn’t too much of a big deal, but over time, there are some side effects to 1) this type of diet pattern and 2) gaining excess body fat.
Excess sodium and body fat are significant contributors to elevated blood pressure (Grillo et al. 2019). Additionally, especially as someone begins to gain a lot of body fat around their midsection (which can be quite common in the bodybuilding or powerlifting population who are focused solely on “eat big to get big”), additional complications such as insulin resistance (on the path to type 2 diabetes), dyslipidemia, and more (Shah et al. 2014) can become bigger concerns. Therefore, in summary, while you could be helping someone achieve one goal (weight gain), the path by which you get there and the extent of the weight gain may lead to unwanted trade-offs.
Injury Example

Finally, this is a pretty simple one, as it comes down to the basics of training planning. While someone may make some short-term progress in muscle or strength with a large spike in training volume, this can also come with an increased risk of injury. As a rule of thumb, the greater the change in training volume vs what you have been used to in the previous 1-3 months, the greater the increase in risk of injury. For example, even if you have done 30 sets for quads in a session in the 6-12 months prior, that doesn’t mean you will be able to tolerate that if you have been performing no quad training or far less volume in the last 3 months.
Therefore, the goal as a coach should not be to build a programme that is going to “destroy” your client and leave them feeling really sore. While that may satisfy the client initially, it comes at the expense of an appropriate training programme, which is very different to one that is just “hard”. In summary, focus on finding an appropriate level of training volume and/or intensity, rather than just thinking more/harder is better.
More to Consider…
There are many more examples that we could discuss, some of which lie in much more grey areas and wrestle directly with some of the points shared above. Here are some additional points to consider…
What about attitudes & beliefs?
How might my advice modify someone’s attitudes/beliefs? Is my advice aligned with a specific narrative, and if so, is that a helpful one? How might this affect the way that someone views their health and fitness behaviours, and the other areas of their life?
Example: If I tell someone that they need to do specific exercises for their posture, one would assume that this aligns with the general narrative relating to posture and pain. This has the potential to reinforce preconceived notions about slouching and back pain, rounded shoulders being harmful etc.. Therefore, I must consider 1) the utility of the advice, and 2) the narrative that runs with it.
What about time?
How much time is going to be invested by the person if I give them this advice? If so, is it likely that the person has this much time available? If so, is this the most time-efficient way for this person to move closer toward the goals they have set for themselves?
Example: If someone starts a “stretching routine” [in addition to resistance training] that is to be performed for 30 minutes daily, that is an investment of 3.5 hrs/wk, 14 hrs/mo, or 182 hrs/yr. That is a lot of time, and hence, I would want to know that this is really in line with that person’s goal (e.g. get better at stretching vs reduce injury risk, great for the former, not for the latter).
What about the cost?
Is there any cost to the advice that I am about to give? If so, is it likely that this is within someone’s budget? If so, is this the most cost-effective way for this person to move closer toward the goals that they have set for themselves?
Example: If someone is going to invest in a supplement for “general health”, it would be fair for that person to assume that, based on what I have said, this supplement is a requirement for long-term health. If this costs €40/mo, that is a cost of €480/yr. That is a lot, and hence, I should probably have a pretty strong justification.
Is this actually correct, or am I misinforming my client?
This is a simpler one, but is the information I am providing correct/true? And, how do I know? Is there a very high level of evidence (e.g. systematic reviews/meta-analyses on x intervention in populations similar to my client), or is this simply my opinion? If the justification is weak, then all of the previous questions become even more important. If advice is based on weak, unsubstantiated claims, is also part of an unhelpful narrative, and carries a significant cost and time investment, then that’s probably not great advice.
Example: If I tell someone they need to follow a specific meal plan with specific foods, requiring someone to eat every 3 hours to lose body fat, that’s 1) not justified based on the evidence, 2) potentially harmful to one’s attitudes/beliefs toward nutrition, and 3) a large investment of time (meal prep, specific shopping) and potentially money.
First, Do No Harm
I would argue that a lot of the harm left behind, or, one’s coaching footprint, actually goes unnoticed. It is the fear of certain movements; of food; of weight gain; of living “impure”. It is the belief that for one to be healthy, one must reduce all life decisions to “positive” or “negative” for health.
It is not just an ignorance of health, but also the attitude that health can be viewed through a purely biomedical lens, at the expense of one’s career, relationships, and sense of fulfilment. It is a flawed understanding of the principles of nutrition. It is the misapplication of “feelings” in exercise prescription. It is the debt incurred by one’s monthly supplement bill. It is the fear of not being “perfect”.
Health is complicated and hence so too is coaching with health in mind. As coaches, acknowledging that responsibility can help. If nothing else, simply ask the question “what am I leaving behind?”.
Look beyond the transformation photo.
Coaching Footprint Summary
They are the basic pillars of my thought process. There are more questions you could ask yourself, but my intent is not to create a standardised list of questions. Rather, I hope that, if you are a coach, you can begin to work on reducing your coaching footprint.
If you are not a coach, then this article can still be equally as valuable. Whose “footprints” have affected you? There are undoubtedly attitudes and beliefs that you hold as a result of social media, the mainstream media, popular books etc. that have shaped a false understanding of lots of things.
If you are a coach who is interested in upskilling and becoming more confident in your ability to coach nutrition, then consider doing our Nutrition Coaching Certification program. If you aren’t a coach already, and want to become a coach, then getting certified to coach nutrition will be a massive benefit to your career.
References & Further Reading
Grillo, A., Salvi, L., Coruzzi, P., Salvi, P., & Parati, G. (2019). Sodium Intake and Hypertension. Nutrients, 11(9), 1970. https://doi.org/10.3390/nu11091970
Jan Borén, M John Chapman, Ronald M Krauss, Chris J Packard, Jacob F Bentzon, Christoph J Binder, Mat J Daemen, Linda L Demer, Robert A Hegele, Stephen J Nicholls, Børge G Nordestgaard, Gerald F Watts, Eric Bruckert, Sergio Fazio, Brian A Ference, Ian Graham, Jay D Horton, Ulf Landmesser, Ulrich Laufs, Luis Masana, Gerard Pasterkamp, Frederick J Raal, Kausik K Ray, Heribert Schunkert, Marja-Riitta Taskinen, Bart van de Sluis, Olov Wiklund, Lale Tokgozoglu, Alberico L Catapano, Henry N Ginsberg, Low-density lipoproteins cause atherosclerotic cardiovascular disease: pathophysiological, genetic, and therapeutic insights: a consensus statement from the European Atherosclerosis Society Consensus Panel, European Heart Journal, Volume 41, Issue 24, 21 June 2020, Pages 2313–2330, https://doi.org/10.1093/eurheartj/ehz962
Linardan, J (2019). Causes of Eating Disorders? A Complete Analysis of Risk & Causal Factors. Break Binge Eating. https://breakbingeeating.com/eating-disorders/causes/
Retterstøl, K., Svendsen, M., Narverud, I., & Holven, K. B. (2018). Effect of low carbohydrate high fat diet on LDL cholesterol and gene expression in normal-weight, young adults: A randomized controlled study. Atherosclerosis, 279, 52–61. https://doi.org/10.1016/j.atherosclerosis.2018.10.013
Shah, R. V., Murthy, V. L., Abbasi, S. A., Blankstein, R., Kwong, R. Y., Goldfine, A. B., Jerosch-Herold, M., Lima, J. A., Ding, J., & Allison, M. A. (2014). Visceral adiposity and the risk of metabolic syndrome across body mass index: the MESA Study. JACC. Cardiovascular imaging, 7(12), 1221–1235. https://doi.org/10.1016/j.jcmg.2014.07.017
Taylor R. (2019). Calorie restriction for long-term remission of type 2 diabetes. Clinical medicine (London, England), 19(1), 37–42. https://doi.org/10.7861/clinmedicine.19-1-37