
Dealing with alcohol in the diet can be quite tricky. If we are discussing nutrition in a comprehensive manner, as we are in this article series, we have to deal with alcohol in the diet. In most countries, some amount of alcohol is consumed regularly, and thus forms a key part of the diet.
So, the goal of this article is to help you to better understand alcohol and how it can be incorporated into a healthy diet.
This article is still a part of the larger article series on how to set up the diet. So far in that article series, we have discussed setting up the calories for the diet, how much protein should you eat, how much fat should you eat, how much carbohydrate you should eat, how much fibre you should eat, how much water you should drink and now we turn our attention to alcohol intake.
Before we get stuck in, I would just like to remind you that we offer comprehensive online coaching. So if you need help with your own exercise program or nutrition, don’t hesitate to reach out. If you are a coach (or aspiring coach) and want to learn how to coach nutrition, then consider signing up to our Nutrition Coach Certification course. We do also have an exercise program design course in the works, if you are a coach who wants to learn more about effective program design and how to coach it. We do have other courses available too.
Understanding Alcohol
While it is often glossed over, alcohol is technically a macronutrient just like protein, carbohydrates and fats. So, when discussing the diet, it does need to be discussed. To do this effectively, and then show you how to deal with alcohol in the diet, you need to have a bit of a better understanding of alcohol. However, considering that the body has no need for alcohol, I am going to discuss this much more briefly than I have discussed the other macronutrients.
Alcohol Metabolism
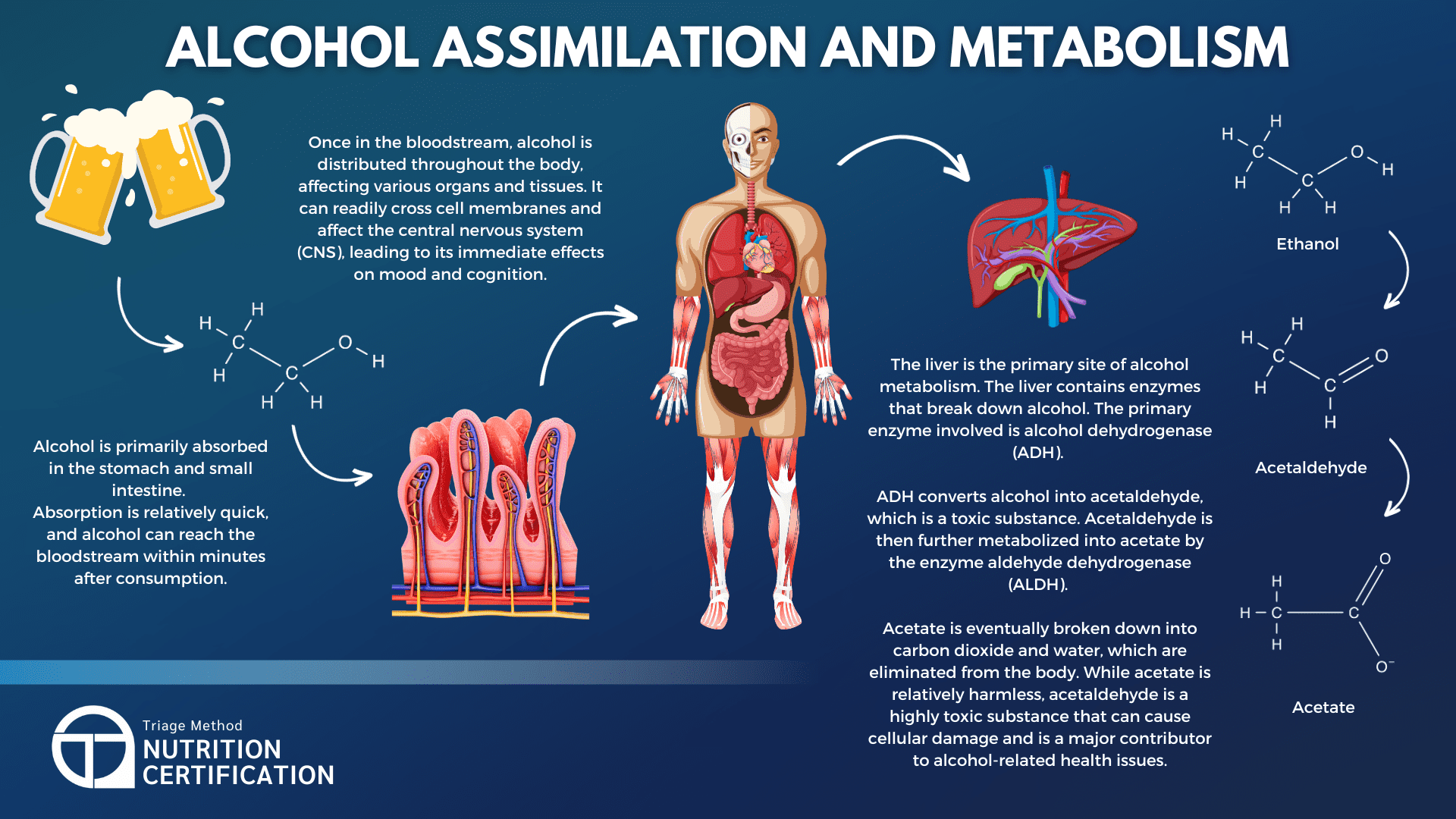
Alcohol is processed by the body in a unique way. When alcohol is consumed, it is absorbed primarily through the stomach and small intestine. Approximately 20% of the alcohol enters the bloodstream through the stomach, while the majority (around 80%) is absorbed in the small intestine.
Factors such as the presence of food in the stomach, the concentration of alcohol in the beverage, and carbonation levels can influence the speed and extent of alcohol absorption. For example, drinking on an empty stomach or consuming carbonated beverages can speed up absorption, leading to quicker intoxication. This is why it is generally recommended to eat a decent meal before drinking.
Once absorbed, alcohol is distributed through the bloodstream to various organs and tissues. Since alcohol is water-soluble, it particularly affects areas with high water content, such as the brain, muscles, and liver. The alcohol travels throughout the body via the blood, leading to changes in mood, behaviour, and motor skills as it interacts with the central nervous system. Blood Alcohol Concentration (BAC) measures the amount of alcohol in the bloodstream, which helps indicate how intoxicated a person is at any given moment.
The liver plays a crucial role in metabolising alcohol. Approximately 90% of alcohol consumed is processed by the liver, where it is broken down by enzymes, primarily alcohol dehydrogenase (ADH) and aldehyde dehydrogenase (ALDH). These enzymes convert alcohol first into acetaldehyde, a toxic compound, and then into acetic acid, which is eventually converted to carbon dioxide and water.
However, the liver can only process a certain amount of alcohol at a time, roughly one standard drink per hour. If alcohol is consumed faster than the liver can metabolise it, the excess alcohol remains in the bloodstream, causing intoxication.
The Effects Of Alcohol
The effects of alcohol on various systems in the body are actually quite profound. The brain, in particular, is significantly impacted. Alcohol is a central nervous system depressant, serving to slow down brain activity. This leads to impaired coordination, judgment, and reaction times, which can be incredibly dangerous in situations like driving.
Most of you have likely been drunk, or have seen people drunk, so I don’t need to elaborate on what alcohol does to your actual function. You likely know that it causes people to basically act like toddlers. They can’t walk or talk properly, they lack impulse control and their coordination isn’t great.
A small amount of alcohol does seem to turn down brain activity just a little bit, which for some people, makes them feel like they can engage better in social situations. At low doses, alcohol also often induces feelings of happiness and relaxation by stimulating dopamine release. Alcohol reduces activity in the prefrontal cortex, the area responsible for judgment and self-control. This can lead to increased sociability and risk-taking behaviour.
This is why alcohol is often called a social lubricant. However, this is largely just a placebo and if anything, alcohol makes you worse at being social (hence all the fighting that occurs when people drink).
Studies using placebo-controlled experiments show that when people believe they’ve consumed alcohol (even if they haven’t), they often report feeling more confident, less inhibited, and more sociable. This suggests that some of alcohol’s effects on sociability are psychological rather than purely chemical. It is a classic case of people prioritising their feelings over the actual facts of the situation.
As blood alcohol concentration increases, motor skills and decision-making start to become affected, leading to clumsiness, slower reaction times, and difficulty focusing. At higher levels of consumption, the slowing of brain activity can make speech difficult to articulate. Excessive drinking can also interfere with the brain’s ability to form memories, leading to partial or complete blackouts.
Alcohol intake also affects the cardiovascular system. Alcohol may cause a temporary increase in heart rate as the body processes the substance. Alcohol dilates blood vessels, particularly in the skin, causing a warm or flushed appearance. This can contribute to a sensation of warmth, even if body temperature is actually dropping.
Alcohol also has a sedative effect, and at higher doses, it can make individuals feel sleepy or lethargic. When paired with the sensation of warmth, it can lead people to lie down outside and go unconscious. This can unfortunately lead to hypothermia and death.
Alcohol also irritates the stomach lining, which can lead to nausea, especially if consumed in large amounts or on an empty stomach. Alcohol relaxes the lower esophageal sphincter, allowing stomach acid to flow back into the esophagus.
Alcohol is a diuretic, meaning it increases urine production. This can contribute to dehydration and electrolyte imbalances.
Alcohol disrupts communication between the brain and muscles, leading to a lack of balance and physical control.
Even short-term alcohol consumption can weaken the immune system’s ability to fight off infections, making individuals more susceptible to illness. While alcohol is not the sole cause of frequent sickness, regular or heavy drinking can impair immune function and contribute to increased vulnerability over time.
Alcohol and The Diet
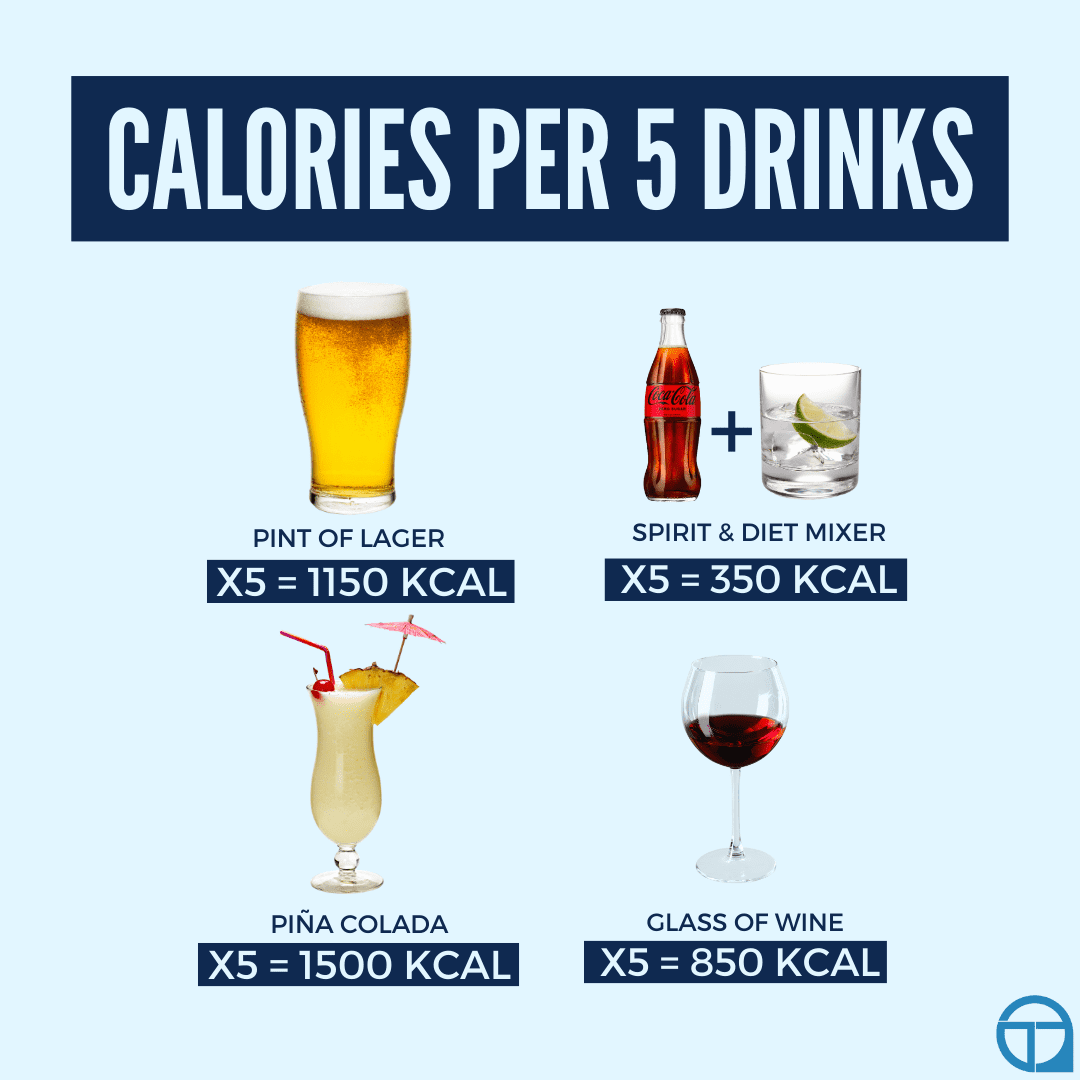
Alcohol unfortunately can contribute significantly to your daily calorie intake. Alcohol provides 7 calories per gram. Unlike other macronutrients, alcohol offers little nutritional value, often referred to as “empty calories.”
The number of calories in alcoholic beverages varies depending on the type of drink and its alcohol content. For instance, beer typically contains around 150 to 200 calories per 355mL serving, with the exact number depending on factors such as the alcohol percentage and the residual sugars in the beer. Wine, in a standard 148mL glass, generally provides between 120 and 150 calories. Spirits, on the other hand, typically contain around 100 calories per 44mL shot. However, when mixed with sugary beverages, these drinks can quickly become calorie-heavy.
When alcohol is consumed, the body prioritises metabolising it over other nutrients. This means that while the liver is busy processing alcohol, fat oxidation (the process by which the body burns fat for energy) is inhibited, leading to an increased likelihood of fat storage.
Chronic alcohol consumption, therefore, can contribute to an increase in body fat, especially around the abdomen, and in the form of visceral fat that is stored around the organs. This fat is particularly concerning because it is associated with an increased risk of metabolic syndrome, type 2 diabetes, and cardiovascular diseases.
While alcohol does provide calories, it generally offers no essential nutrients and actually interferes with the absorption of important vitamins and minerals. The digestive system’s ability to absorb nutrients is compromised when alcohol is consumed. Essential vitamins like thiamine (B1), folate, and vitamin B12, as well as minerals like calcium, magnesium, and zinc, are poorly absorbed during alcohol consumption.
Chronic alcohol use can lead to significant nutrient deficiencies. For example, a lack of thiamine can lead to Wernicke-Korsakoff syndrome, a neurological disorder that affects memory and cognition. Alcohol also depletes magnesium levels, which can result in muscle cramps and other neurological issues. Folate deficiency due to heavy drinking is another common issue, leading to anaemia and complications in DNA synthesis.
Alcohol and Hydration
Alcohol is a diuretic, as it increases urine production by inhibiting the release of antidiuretic hormone (ADH). This leads to greater fluid loss, which contributes to dehydration. Dehydration can result in symptoms like dry mouth, fatigue, and headaches, which as most of you are aware, are commonly experienced as part of a hangover.
Despite feeling like you are hydrating by drinking liquids, when alcohol is consumed, it does actually lead to dehydration. To mitigate this, it is crucial to actively stay on top of your hydration while drinking alcohol.
A strategy I often recommend to my clients is to alternate between alcoholic and non-alcoholic beverages, ideally water. Drinking water before, during, and after alcohol consumption can also help replenish lost fluids. Additionally, consuming drinks with lower alcohol content can reduce the diuretic effect. Electrolyte-rich drinks, such as sports drinks, can also help restore important minerals lost through frequent urination. Aiming to at least cover your baseline water needs is a good idea while drinking.
Understanding how alcohol is metabolised and its impact on the body can help you to make more informed decisions about your drinking habits. However, to be truly informed, we need to actually discuss the long term effects of alcohol consumption on your health.
Alcohol’s Impact on Health
Alcohol consumption, especially when excessive or chronic, has widespread effects on the body and mind. While moderate drinking has been associated with certain potential benefits, these are often overstated, and the risks of overconsumption far outweigh any advantages.
Impact on the Brain and Mental Health
Chronic alcohol use can severely damage critical areas of the brain. The frontal lobe, responsible for decision-making, impulse control, and problem-solving, often suffers from long-term alcohol-related damage. This leads to poor judgment, reduced cognitive flexibility, and impaired social functioning. Similarly, the hippocampus, which plays a key role in memory formation and spatial navigation, is vulnerable to alcohol’s toxic effects. Over time, this can result in significant memory loss and learning difficulties.
One severe neurological consequence of prolonged alcohol consumption is Wernicke-Korsakoff syndrome, a condition caused by thiamine (vitamin B1) deficiency. This syndrome often presents with confusion, memory impairment, and motor coordination problems. Without intervention, it can progress to irreversible brain damage.
Alcohol is also closely linked to mental health disorders. Heavy drinking exacerbates mood disorders, including anxiety and depression, as alcohol disrupts the brain’s chemical balance and alters serotonin and dopamine levels. While alcohol initially acts as a depressant, dampening nervous system activity and potentially numbing negative emotions, these effects are temporary and deceptive. Over time, alcohol disrupts brain chemistry, creating or amplifying emotional instability and deepening the severity of mental health challenges.
While people may turn to alcohol as a temporary escape from negative emotions, this often creates a vicious cycle of dependency and worsened mental health. Over time, dependency on alcohol can develop, leading to addiction, withdrawal symptoms, and significant social and psychological consequences.
Effects on the Liver
The liver is perhaps the organ most heavily impacted by chronic alcohol use, as it is responsible for metabolising the majority of alcohol consumed. Over time, excessive drinking can lead to a range of liver conditions:
- Fatty Liver Disease: This is the earliest stage of liver damage, characterised by the accumulation of fat in liver cells. It is often reversible with abstinence but can progress if drinking continues.
- Alcoholic Hepatitis: Prolonged heavy drinking can cause inflammation of the liver, leading to symptoms such as jaundice, abdominal pain, and fatigue.
- Cirrhosis: In severe cases, liver tissue becomes scarred and permanently damaged, impairing the liver’s ability to detoxify the body, metabolise nutrients, and store essential vitamins and minerals.
These conditions not only harm overall health but also increase the risk of liver failure and death.
Cardiovascular Effects
The relationship between alcohol and heart health is complex. In moderation, certain types of alcohol, such as red wine, have been associated with modest cardiovascular benefits, including increased HDL (the “good” cholesterol) and improved blood flow. However, these benefits are seriously overblown and often used to justify drinking without considering the risks.
Excessive alcohol consumption significantly increases the risk of:
- High Blood Pressure: Alcohol raises blood pressure, potentially straining the cardiovascular system.
- Arrhythmias: Irregular heartbeats can result from heavy drinking, contributing to long-term heart issues.
- Cardiomyopathy: This disease weakens the heart muscle, reducing its ability to pump blood effectively.
- Stroke: Both ischemic and hemorrhagic strokes are more common in heavy drinkers due to alcohol’s effects on blood pressure and clotting abilities.
Gastrointestinal and Pancreatic Health
Alcohol irritates and inflames the digestive system. It is a known cause of gastritis and can exacerbate conditions like acid reflux by weakening the lower esophageal sphincter. Chronic drinking may also lead to ulcers and other complications related to the stomach lining.
The pancreas is another organ vulnerable to alcohol’s toxic effects. Prolonged heavy drinking increases the risk of pancreatitis, a painful and potentially life-threatening condition caused by inflammation of the pancreas. Pancreatitis can occur acutely after binge drinking or develop into a chronic issue with repeated alcohol exposure.
Weakened Immune Function
Alcohol suppresses the immune system, making the body more susceptible to infections. Chronic heavy drinking impairs the production and activity of white blood cells, weakening the body’s defences. This is particularly concerning for individuals who drink heavily over long periods, as they are more prone to illnesses like pneumonia, tuberculosis, and other infections.
Alcohol and Cancer
Alcohol is a known carcinogen, and its consumption increases the risk of several types of cancer. The risk is dose-dependent, meaning the more alcohol consumed, the greater the likelihood of developing cancer.
There are a variety of cancers directly attributed to alcohol intake, such as:
- Oral and Throat Cancers: Alcohol irritates the lining of the mouth, throat, and esophagus, increasing cancer risk. The risk is compounded when combined with smoking.
- Liver Cancer: Chronic alcohol use can lead to cirrhosis, which significantly raises the risk of liver cancer.
- Breast Cancer: Even moderate alcohol consumption is associated with an increased risk of breast cancer, likely due to alcohol’s effect on estrogen levels.
- Colorectal Cancer: Alcohol consumption increases the risk of cancers in the colon and rectum.
There are a variety of potential mechanisms behind why alcohol can increase cancer risk, including:
- Acetaldehyde Production: When alcohol is metabolised, it produces acetaldehyde, a toxic compound that damages DNA and proteins.
- Oxidative Stress: Alcohol metabolism generates free radicals, which can damage cells and increase cancer risk.
- Hormonal Changes: Alcohol can increase levels of hormones like estrogen, which are linked to hormone-sensitive cancers such as breast cancer.
- Weakened Immune Function: Alcohol weakens the immune system, and the immune system is responsible for dealing with cancer.
Even light drinking carries some risk, with no truly “safe” level of alcohol consumption when it comes to cancer risk.
Alcohol and Overall Longevity and Mortality
The relationship between alcohol and overall longevity depends on the amount and frequency of consumption.
Moderate Drinking and Longevity
Some studies suggest that moderate alcohol consumption is associated with a slightly lower risk of all-cause mortality compared to heavy drinking or complete abstinence. This “J-shaped curve” is often cited to support moderate drinking, with proposed mechanisms including cardiovascular benefits and social factors.
However, more recent research challenges this finding, suggesting that the apparent benefits of moderate drinking may be due to confounding factors such as lifestyle, socioeconomic status, or preexisting health conditions in non-drinkers (i.e. non-drinkers may not drink because they are sick or at risk).
Heavy Drinking and Reduced Lifespan
Excessive alcohol consumption is strongly associated with increased mortality and a shorter lifespan. This is due to:
- Increased risk of chronic diseases (e.g., liver disease, cancer, and heart disease).
- Higher likelihood of injuries and accidents caused by impaired judgment.
- Greater susceptibility to infections due to weakened immune function.
Binge Drinking and Mortality
Even occasional binge drinking significantly increases the risk of sudden death from alcohol poisoning, heart arrhythmias, and accidents. It also contributes to long-term health issues when repeated over time.
No Safe Level Of Alcohol Intake
In moderation, alcohol (particularly red wine) has been linked to some health benefits, such as improved cardiovascular health due to its antioxidant properties (e.g., resveratrol). However, these effects are often exaggerated, and the risks of overconsumption far outweigh any modest benefits. For individuals who do not already drink, there is no health-based reason to start.
A growing body of research suggests that the risks of alcohol consumption outweigh any potential benefits for overall longevity. Even low to moderate alcohol use may slightly increase the risk of certain diseases, particularly cancer. Drinking any amount of alcohol is likely to reduce your health and overall longevity.
Alcohol and Health
The long-term effects of alcohol are wide-ranging and predominantly harmful, impacting nearly every major organ system in the body as well as mental health. While moderate drinking may carry some potential benefits, these are largely overstated and do not justify the risks associated with overconsumption.
To protect overall health, you should approach alcohol with caution, prioritising moderation or abstinence, particularly if you have any underlying health concerns or a predisposition to addiction.
The Psychology of Drinking Alcohol
Before I elaborate on how to deal with alcohol in the diet, I do just want to briefly touch on the psychology behind alcohol consumption. Understanding this does help you to better understand why you drink alcohol, and thus allows you to actually make better decisions around your own alcohol intake.
Alcohol consumption is deeply rooted in human behaviour and influenced by a range of social, psychological, and cultural factors. People drink for various reasons, often tied to their environment, mental state, and cultural norms.
Reasons People Drink
Social motivations are among the most common reasons for drinking. Alcohol is often seen as a social lubricant, easing interactions and helping individuals feel more relaxed in group settings. It is a staple at celebrations, rituals, and communal gatherings in many cultures.
Psychologically, people may drink to cope with stress, anxiety, or negative emotions, seeking temporary relief from their mental state. Others drink for pleasure, as alcohol stimulates the release of dopamine, creating feelings of reward and enjoyment.
Cultural influences also play a significant role, as societal norms dictate how, when, and why alcohol is consumed. In some cultures, drinking is deeply ingrained in traditions, while in others, it may be stigmatised or prohibited.
Patterns of Alcohol Use
We can also categorise alcohol consumption into different patterns of use, and again, understanding your own pattern of use helps you to make better, more informed decisions around dealing with alcohol in the diet.
- Occasional Drinking: Individuals who drink sporadically, often during special events or celebrations, without significant consequences or dependency.
- Moderate Regular Drinking: Regular but controlled consumption that aligns with health guidelines (e.g., up to one drink per day for women, two for men). This pattern is typically not associated with harm.
- Excessive Drinking: Includes binge drinking (consuming large amounts in a short time) and chronic heavy drinking. These patterns carry significant risks, including addiction, health complications, and social consequences.
Of course, there is also abstinence, but this isn’t really a pattern of use, and is instead a pattern of non-use.
Assessing Your Own Reasons and Patterns Of Use
Understanding why you drink and identifying your pattern of alcohol use can be really helpful in maintaining a healthy relationship with alcohol. Self-awareness allows you to evaluate whether your consumption aligns with your goals, values, and overall well-being, and whether it may pose risks to your physical or mental health.
This is something I often have to go through with clients, which usually involves a good bit of back and forth, but I have tried to lay out the basic framework for this below.
Exploring Your Motivations
Reflecting on why you consume alcohol can provide very valuable insights into your alcohol use. Are you drinking for social connection? To enhance celebrations? Or to relax after a long day? Perhaps you use alcohol to manage stress, cope with difficult emotions, or alleviate boredom?
These underlying motivations can reveal whether your drinking is a conscious choice or a coping mechanism for deeper issues. If the latter, addressing the root causes through alternative strategies (such as mindfulness, therapy, or even physical activity) can be beneficial.
Recognising Your Pattern of Use
Determining where your habits fall within the spectrum of alcohol use (occasional, moderate, or excessive) can help you make informed decisions. For example:
- If you’re an occasional drinker, you might already have a balanced relationship with alcohol (unless you are binge drinking occasionally).
- Moderate drinkers can benefit from tracking their intake to ensure they stay within healthy guidelines (which I will discuss more in a moment).
- If you identify with excessive drinking, it may be time to evaluate the impact on your health, relationships, and productivity, and consider reducing consumption or seeking support.
Questions to Ask Yourself
To better understand your relationship with alcohol, consider these questions:
- How often do I drink, and how much do I consume?
- Do I feel pressure to drink in social situations, or can I abstain comfortably?
- Am I using alcohol to escape stress, sadness, or other negative emotions?
- Has my alcohol use negatively impacted my health, relationships, or responsibilities?
By reflecting on these questions, you can identify whether your drinking habits align with your actual intentions, goals and ideal life. You can then assess whether any changes might be beneficial.
Balanced Approach To Alcohol Intake
If your evaluation reveals areas of concern, small changes can lead to significant improvements here. Setting clear boundaries, such as limiting the number of drinks or choosing alcohol-free days, can reduce risks while preserving the social or enjoyable aspects of drinking.
If you find it challenging to make changes, seeking professional guidance can provide the tools and support needed to address underlying issues and establish healthier habits.
But how much alcohol is actually an acceptable and OK amount of alcohol to consume?
How Much Alcohol Should You Drink?
All of you are aware that alcohol isn’t exactly healthy to consume and it leads to major health issues if consumed frequently and in excessive quantities. What is surprising to most, however, is just how low the recommended maximum daily/weekly alcohol consumption targets are, especially if you are from a culture where people drink a lot.
High alcohol intakes are normalised in many parts of the world, but that, unfortunately, doesn’t mean that this is not having ill effects on health. Most people are going to see ill health effects from intakes that are seen as normal, and people very often knock years off their life both in terms of quantity and quality (poor sleep as a result of alcohol causing you to underperform in daily life is an incredibly common phenomenon).
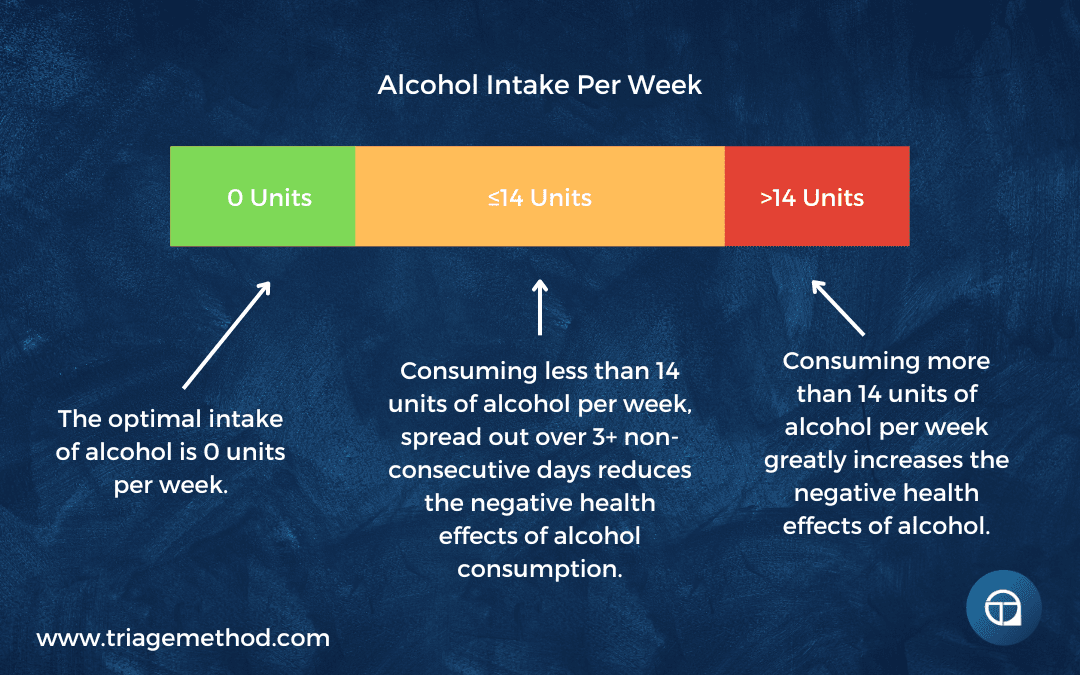
The guidelines differ from country to country, but a very rough target is 14 units per week, with one unit being 8-10g of actual alcohol.
If consuming the 14 units in a week, it is advised that this is spread out over at least three days, ideally non-consecutive days. More than this is generally seen as problematic and begins getting into the territory of alcohol dependence syndrome/alcoholism.
| Country | Standard Drink Definition | Recommended Limits for Men | Recommended Limits for Women | Units Per Week | Additional Notes |
|---|---|---|---|---|---|
| Australia | 10 grams of ethanol | Up to 40g per day; no more than 100g per week | Same as men | ~10 units | Encourages at least two alcohol-free days per week. |
| Austria | 20 grams of ethanol | Up to 24g per day | Up to 16g per day | ~12 units (men), ~8 units (women) | Recommends two alcohol-free days per week. |
| Canada | 13.6 grams of ethanol | Up to 27g per week | Same as men | ~2 units | Advises that not drinking has benefits, such as better health and sleep. |
| Denmark | 12 grams of ethanol | Up to 48g per day; no more than 120g per week | Same as men | ~10 units | Suggests limiting alcohol intake to reduce health risks. |
| Finland | 12 grams of ethanol | Up to 168g per week | Up to 84g per week | ~14 units (men), ~7 units (women) | Emphasizes the importance of moderation to minimize health risks. |
| Germany | 10-12 grams of ethanol | Avoid alcohol completely if possible | Avoid alcohol completely if possible | No recommended units | Recommendations focus on reducing alcohol consumption regardless of amount. |
| Ireland | 10 grams of ethanol | Up to 170g per week | Up to 140g per week | ~17 units (men), ~14 units (women) | Advises spreading drinking over the week and having some alcohol-free days. |
| Italy | 12 grams of ethanol | Up to 24g per day | Up to 12g per day | ~14 units (men), ~7 units (women) | Recommends drinking during meals and avoiding binge drinking. |
| Japan | 19.75 grams of ethanol | Up to 40g per day | Up to 20g per day | ~20 units (men), ~10 units (women) | Encourages moderation and awareness of alcohol’s effects on health. |
| Netherlands | 10 grams of ethanol | Advises no alcohol or one glass daily | Advises no alcohol or one glass daily | ~10 units | The Health Council included this in the Dutch Dietary Guidelines 2015. |
| New Zealand | 10 grams of ethanol | Up to 30g per day; no more than 150g per week | Up to 20g per day; no more than 100g per week | ~15 units (men), ~10 units (women) | Recommends at least two alcohol-free days per week. |
| Norway | 12 grams of ethanol | Up to 20g per day | Up to 10g per day | ~11 units (men), ~5.5 units (women) | Suggests limiting alcohol intake to reduce health risks. |
| United States | 14 grams of ethanol | Up to 28g per day | Up to 14g per day | ~14 units (men), ~7 units (women) | Defines moderate drinking as up to two drinks per day for men and one for women. |
I know that isn’t what people like to hear, and as soon as they hear it, they come up with all kinds of excuses as to why their alcohol use is not problematic and that they just have a glass or two of wine/beer each night to wind down. However, this is the guideline for a reason, and even this level of intake isn’t risk-free or even safe, it is just considered to be lower risk.
There are certainly cases to be made to decrease or increase this guideline, depending on your genetics and size. However, we are talking about decreasing/increasing by about 1 unit either way (13-15 units per week), and for the vast majority of people, a stronger case can be made that very low or zero intake would be better for health.
To put it in perspective, here is the breakdown of some common alcoholic beverages and their units of alcohol:
Beer: Common alcohol content is 3.5-5.5% ABV, so one pint (568mL) is about 3 units. (Stronger/weaker beers will obviously make this number variable, but you can think of a pint to be between 2-4 units). So roughly 3.5-6 pints depending on the strength is 14 units of alcohol.
Wine: A medium glass (175mL) has roughly 2 units. Some wines, especially red, are higher percentage alcohol though, and for the same amount (volume) so this can be as high as 3 units. It is easier to think in terms of a bottle of wine, a 750mL bottle of 12% ABV has about 9 units, while a 16% ABV wine has about 12 units. So between 1 and a half bottles, and 1 bottle and a medium glass of wine is 14 units of alcohol.
Spirits: At roughly 40% ABV, a shot of spirits is between 1 and 1.5 units, depending on the size of the shot (it can vary between 25-35mL). So roughly 9-14 shots is 14 units of alcohol.
Alcopops: These vary quite a bit, depending on the exact alcohol in question, but a rough figure of between 1 and 1.5 units is where they are commonly thought to be. Again, roughly 9-14 alcopops is 14 units of alcohol.
You more than likely know people who regularly consume more than this regularly (or you may even do so yourself). Unfortunately, even this seemingly low level of intake (I think it is fair to say that most people would consider ~4 pints of beer or 1.5 bottles of wine per week to be quite low) is at the very limit of what is low-risk. Even this level is not safe. It is especially not safe if you drink and drive, both for you and those around you.
Fitting Alcohol Into The Diet
Anyway, this is not an article about getting you to be abstinent, even if that would be better for your health, performance and body composition. What you want to know is how to fit alcohol into the diet.
Alcohol itself contains ~7 calories per gram, and when looking to fit alcohol into the diet, we generally just substitute carbs and fats for alcohol. So if you want to have a glass of wine, you would simply account for the calories, subtracting them from the calories you have allocated to carbs and/or fat.
Ideally, you would consume the alcohol away from sleep, as it generally reduces sleep quality. The reduced sleep quality also tends to make the diet, training and general life harder the next day(s). You would also, ideally, stay below the 14 units of alcohol per week, if you want to reduce the various health risks associated with alcohol intake.
As some of you will want to drink more on maybe a single day, you may soon realise that you can’t fit that amount of calories into your overall plan. We can deal with this similarly to dealing with meals at events where we know we will be consuming more calories than would normally fit in our diet. It can help to view your calories over the week, rather than only for a single day.
It is calorie intake over time that dictates results, so looking at things across the week, rather than a single day can help us to even out the calorie average. So if you want to consume more on a Saturday, you may just consume slightly less across the rest of the week, to allow for more calories on that Saturday. Eating 100 fewer calories Monday to Friday will allow you to consume 500 extra calories on that Saturday, and assuming your Sunday intake is where it normally would be, your weekly average calorie intake will be the same.
However, this is usually an incredibly slippery slope, especially when dieting. Most people will try this method and just end up hungrier across the week, and then end up binge eating on the Saturday because they have felt so restricted. This is especially the case when you also add alcohol to the mix.
This still happens even when the calories saved through the week aren’t even that high. So a better way of dealing with events like this is to simply drink less alcohol. I know that isn’t the answer you want, but unfortunately, it isn’t easy to deal with alcohol in the diet unless you engage in practices that aren’t generally conducive to a good diet.
Ideally, you would still prioritise consuming sufficient protein on the days when more of your calories are coming from alcohol. Just because you are drinking alcohol doesn’t mean you no longer need enough protein.
While alcohol is not very health promoting (and is in fact, bad for your health) if you account for the calories in it and consume enough protein, you can reduce the harm and keep your diet more on track.
Quick Summary: Ideally, consume zero alcohol, but if you must consume it, aim to consume less than 14 units of alcohol per week, spread out over at least 3 (ideally non-consecutive) days. Account for the calories of the drinks you consume, substituting out fats and/or carbs to allow for the alcohol intake.
Dealing With Alcohol In The Diet Conclusion
I know that a lot of people are very often surprised at just how little alcohol they should be drinking. Most people are aware that alcohol is not great for them, but I know from coaching lots of people, that most people do also want to incorporate alcohol into their diet in some manner.
So, hopefully, this article has helped you to understand alcohol a bit better and helped you to think about dealing with alcohol in your diet.
Dietary change does just take some time and effort. If you need help with this, you can always reach out to us and get online coaching, or alternatively, you can interact with our free content.
If you want more free information on nutrition, you can follow us on Instagram, YouTube or listen to the podcast, where we discuss all the little intricacies of exercise and nutrition. You can always stay up to date with our latest content by subscribing to our newsletter.
Finally, if you want to learn how to coach nutrition, then consider our Nutrition Coach Certification course, and if you want to learn to get better at exercise program design, then consider our course on exercise program design. We do have other courses available too. If you don’t understand something, or you just need clarification, you can always reach out to us on Instagram or via email.
The previous article in this series is about How Much Water Should You Drink? and the next article in this series is Overview of Diet Quantity, if you are interested in continuing to learn about nutrition. You can also go to our nutrition hub to find more nutrition content.
References and Further Reading
A Review of the Effects of Alcohol on Carbohydrate Metabolism. (1977). Alcohol and Alcoholism. http://doi.org/10.1093/oxfordjournals.alcalc.a044072
Paton, A. (2005). Alcohol in the body. Bmj, 330(7482), 85–87. http://doi.org/10.1136/bmj.330.7482.85
Jorfeldt, L., & Juhlin-Dannfelt, A. (1978). The influence of ethanol on splanchnic and skeletal muscle metabolism in man. Metabolism, 27(1), 97–106. http://doi.org/10.1016/0026-0495(78)90128-2
Preedy, V. R., Reilly, M. E., Patel, V. B., Richardson, P. J., & Peters, T. J. (1999). Protein metabolism in alcoholism: effects on specific tissues and the whole body. Nutrition, 15(7-8), 604–608. http://doi.org/10.1016/s0899-9007(99)00096-9
Rachdaoui, N., & Sarkar, D. K. (2013). Effects of Alcohol on the Endocrine System. Endocrinology and Metabolism Clinics of North America, 42(3), 593–615. http://doi.org/10.1016/j.ecl.2013.05.008
Colrain, I. M., Nicholas, C. L., & Baker, F. C. (2014). Alcohol and the sleeping brain. Handbook of Clinical Neurology Alcohol and the Nervous System, 415–431. http://doi.org/10.1016/b978-0-444-62619-6.00024-0
Ebrahim, I. O., Shapiro, C. M., Williams, A. J., & Fenwick, P. B. (2013). Alcohol and Sleep I: Effects on Normal Sleep. Alcoholism: Clinical and Experimental Research, 37(4). http://doi.org/10.1111/acer.12006
I, V. E., & M, M. J. (1970). Alcohol, Amines, and Alkaloids: A Possible Biochemical Basis for Alcohol Addiction. Science, 167(3920), 1005–1007. http://doi.org/10.1126/science.167.3920.1005
Quertemont E, Didone V. Role of acetaldehyde in mediating the pharmacological and behavioral effects of alcohol. Alcohol Res Health. 2006;29(4):258‐265. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6527032/
Lieber, C. (1980). Alcohol, liver injury and protein metabolism. Pharmacology Biochemistry and Behavior, 13, 17–30. http://doi.org/10.1016/s0091-3057(80)80004-9
Goel, S., Sharma, A., & Garg, A. (2018). Effect of Alcohol Consumption on Cardiovascular Health. Current Cardiology Reports, 20(4). http://doi.org/10.1007/s11886-018-0962-2
Burke, L. M., Collier, G. R., Broad, E. M., Davis, P. G., Martin, D. T., Sanigorski, A. J., & Hargreaves, M. (2003). Effect of alcohol intake on muscle glycogen storage after prolonged exercise. Journal of Applied Physiology, 95(3), 983–990. http://doi.org/10.1152/japplphysiol.00115.2003
Dasarathy, J., Mccullough, A. J., & Dasarathy, S. (2017). Sarcopenia in Alcoholic Liver Disease: Clinical and Molecular Advances. Alcoholism: Clinical and Experimental Research, 41(8), 1419–1431. http://doi.org/10.1111/acer.13425
Trevejo-Nunez G, Kolls JK, de Wit M. Alcohol Use As a Risk Factor in Infections and Healing: A Clinician’s Perspective. Alcohol Res. 2015;37(2):177‐184. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4590615/
https://www.who.int/news-room/fact-sheets/detail/alcohol
https://alcoholireland.ie/download/publications/Crime%20Briefing%20Final.pdf
https://www.drugsandalcohol.ie/15781/1/HSE_Costs_to_Society_of_Problem_Alcohol_Use_in_Ireland.pdf
Rivlin RS. Magnesium deficiency and alcohol intake: mechanisms, clinical significance and possible relation to cancer development (a review). J Am Coll Nutr. 1994;13(5):416-423. doi:10.1080/07315724.1994.10718430 https://pubmed.ncbi.nlm.nih.gov/7836619/
Lieber, C. S. (2009). The Influence of Alcohol on Nutritional Status. Nutrition Reviews, 46(7), 241–254. http://doi.org/10.1111/j.1753-4887.1988.tb05443.x
Klatskin, G., & Krehl, W. A. (1954). The Effect Of Alcohol On The Choline Requirement. The Journal of Experimental Medicine, 100(6), 615–627. http://doi.org/10.1084/jem.100.6.615
Loguercio, C., Piscopo, P., Guerriero, C., Girolamo, V. D., Disalvo, D., & Blanco, C. D. V. (1996). Effect of alcohol abuse and glutathione administration on the circulating levels of glutathione and on antipyrine metabolism in patients with alcoholic liver cirrhosis. Scandinavian Journal of Clinical and Laboratory Investigation, 56(5), 441–447. http://doi.org/10.3109/00365519609088799
Kerksick, C., & Willoughby, D. (2005). The Antioxidant Role of Glutathione and N-Acetyl-Cysteine Supplements and Exercise-Induced Oxidative Stress. Journal of the International Society of Sports Nutrition, 2(2). http://doi.org/10.1186/1550-2783-2-2-38
Mosbah, I. B., Alfany-Fernández, I., Martel, C., Zaouali, M. A., Bintanel-Morcillo, M., Rimola, A., … Peralta, C. (2010). Endoplasmic reticulum stress inhibition protects steatotic and non-steatotic livers in partial hepatectomy under ischemia–reperfusion. Cell Death & Disease, 1(7). http://doi.org/10.1038/cddis.2010.29
Henzel, K., Thorborg, C., Hofmann, M., Zimmer, G., & Leuschner, U. (2004). Toxicity of ethanol and acetaldehyde in hepatocytes treated with ursodeoxycholic or tauroursodeoxycholic acid. Biochimica Et Biophysica Acta (BBA) – Molecular Cell Research, 1644(1), 37–45. http://doi.org/10.1016/j.bbamcr.2003.10.017
Corbin, K. D., & Zeisel, S. H. (2012). Choline metabolism provides novel insights into nonalcoholic fatty liver disease and its progression. Current Opinion in Gastroenterology, 28(2), 159–165. http://doi.org/10.1097/mog.0b013e32834e7b4b
Mcclain, C. J., Hill, D. B., Song, Z., Chawla, R., Watson, W. H., Chen, T., & Barve, S. (2002). S-Adenosylmethionine, cytokines, and alcoholic liver disease. Alcohol, 27(3), 185–192. http://doi.org/10.1016/s0741-8329(02)00224-0
Laufer, E. M., Hartman, T. J., Baer, D. J., Gunter, E. W., Dorgan, J. F., Campbell, W. S., … Taylor, P. R. (2004). Effects of moderate alcohol consumption on folate and vitamin B12 status in postmenopausal women. European Journal of Clinical Nutrition, 58(11), 1518–1524. http://doi.org/10.1038/sj.ejcn.1602002
Soyka, M., Kranzler, H. R., Hesselbrock, V., Kasper, S., Mutschler, J., & Möller, H.-J. (2016). Guidelines for biological treatment of substance use and related disorders, part 1: Alcoholism, first revision. The World Journal of Biological Psychiatry, 18(2), 86–119. http://doi.org/10.1080/15622975.2016.1246752
Gong, Y.-S., Hu, K., Yang, L.-Q., Guo, J., Gao, Y.-Q., Song, F.-L., … Liang, C.-Y. (2017). Comparative effects of EtOH consumption and thiamine deficiency on cognitive impairment, oxidative damage, and β-amyloid peptide overproduction in the brain. Free Radical Biology and Medicine, 108, 163–173. http://doi.org/10.1016/j.freeradbiomed.2017.03.019
Hoyumpa, A. M. (1980). Mechanisms of thiamin deficiency in chronic alcoholism. The American Journal of Clinical Nutrition, 33(12), 2750–2761. http://doi.org/10.1093/ajcn/33.12.2750
Rees, E., & Gowing, L. R. (2012). Supplementary Thiamine is Still Important in Alcohol Dependence. Alcohol and Alcoholism, 48(1), 88–92. http://doi.org/10.1093/alcalc/ags120
Rosenthal, W. S., Adham, N. F., Lopez, R., & Cooperman, J. M. (1973). Riboflavin deficiency in complicated chronic alcoholism. The American Journal of Clinical Nutrition, 26(8), 858–860. http://doi.org/10.1093/ajcn/26.8.858
Dutta, P., Seirafi, J., Halpin, D., Pinto, J., & Rivlin, R. (1995). Acute ethanol exposure alters hepatic glutathione metabolism in riboflavin deficiency. Alcohol, 12(1), 43–47. http://doi.org/10.1016/0741-8329(94)00068-o
Vech, R. L., Lumeng, L., & Li, T. K. (1975). Vitamin B6 metabolism in chronic alcohol abuse The effect of ethanol oxidation on hepatic pyridoxal 5-phosphate metabolism. Journal of Clinical Investigation, 55(5), 1026–1032. http://doi.org/10.1172/jci108003
Lumeng, L., & Li, T.-K. (1974). Vitamin B6 Metabolism in Chronic Alcohol Abuse. Journal of Clinical Investigation, 53(3), 693–704. http://doi.org/10.1172/jci107607
Sanvisens, A., Zuluaga, P., Pineda, M., Fuster, D., Bolao, F., Juncà, J., … Muga, R. (2017). Folate deficiency in patients seeking treatment of alcohol use disorder. Drug and Alcohol Dependence, 180, 417–422. http://doi.org/10.1016/j.drugalcdep.2017.08.039
Wani, N. A., Thakur, S., Najar, R. A., Nada, R., Khanduja, K. L., & Kaur, J. (2013). Mechanistic insights of intestinal absorption and renal conservation of folate in chronic alcoholism. Alcohol, 47(2), 121–130. http://doi.org/10.1016/j.alcohol.2012.11.003
Wani, N. A., Nada, R., Khanduja, K. L., & Kaur, J. (2012). Decreased activity of folate transporters in lipid rafts resulted in reduced hepatic folate uptake in chronic alcoholism in rats. Genes & Nutrition, 8(2), 209–219. http://doi.org/10.1007/s12263-012-0318-2
Lindenbaum, J., & Lieber, C. S. (1969). Alcohol-induced Malabsorption of Vitamin B12 in Man. Nature, 224(5221), 806–806. http://doi.org/10.1038/224806a0
Waly, M. I., Kharbanda, K. K., & Deth, R. C. (2010). Ethanol Lowers Glutathione in Rat Liver and Brain and Inhibits Methionine Synthase in a Cobalamin-Dependent Manner. Alcoholism: Clinical and Experimental Research, 35(2), 277–283. http://doi.org/10.1111/j.1530-0277.2010.01343.x
Rivlin, R. S. (1994). Magnesium deficiency and alcohol intake: mechanisms, clinical significance and possible relation to cancer development (a review). Journal of the American College of Nutrition, 13(5), 416–423. http://doi.org/10.1080/07315724.1994.10718430
Sobral-Oliveira, M. B., Faintuch, J., Guarita, D. R., Oliveira, C. P., & Carrilho, F. J. (2011). Nutritional profile of asymptomatic alcoholic patients. Arquivos De Gastroenterologia, 48(2), 112–118. http://doi.org/10.1590/s0004-28032011000200006
Ordak, M., Maj-Zurawska, M., Matsumoto, H., Bujalska-Zadrozny, M., Kieres-Salomonski, I., Nasierowski, T., … Wojnar, M. (2017). Ionized magnesium in plasma and erythrocytes for the assessment of low magnesium status in alcohol dependent patients. Drug and Alcohol Dependence, 178, 271–276. http://doi.org/10.1016/j.drugalcdep.2017.04.035
Romani AM. Magnesium homeostasis and alcohol consumption. Magnes Res. 2008;21(4):197‐204. https://pubmed.ncbi.nlm.nih.gov/19271417/
Belknap, J., Berg, J., & Coleman, R. (1978). Alcohol withdrawal and magnesium deficiency in mice. Pharmacology Biochemistry and Behavior, 9(1), 1–6. http://doi.org/10.1016/0091-3057(78)90003-5
Mullins, P. G. M., & Vink, R. (1995). Chronic alcohol exposure decreases brain intracellular free magnesium concentration in rats. NeuroReport, 6(12), 1633–1636. http://doi.org/10.1097/00001756-199508000-00011
Elisaf, M., Merkouropoulos, M., Tsianos, E., & Siamopoulos, K. (1995). Pathogenetic Mechanisms of Hypomagnesemia in Alcoholic Patients. Journal of Trace Elements in Medicine and Biology, 9(4), 210–214. http://doi.org/10.1016/s0946-672x(11)80026-x
KLINGMAN WO, SUTER C, GREEN R, ROBINSON I. Role of alcoholism and magnesium deficiency in convulsions. Trans Am Neurol Assoc. 1955;(80th Meeting):162‐165. https://pubmed.ncbi.nlm.nih.gov/13312029/
Prior, P. L., & Galduróz, J. C. F. (2011). Glutamatergic hyperfunctioning during alcohol withdrawal syndrome: Therapeutic perspective with zinc and magnesium. Medical Hypotheses, 77(3), 368–370. http://doi.org/10.1016/j.mehy.2011.05.017
Peake, R., Godber, I., & Maguire, D. (2013). The effect of magnesium administration on erythrocyte transketolase activity in alcoholic patients treated with thiamine. Scottish Medical Journal, 58(3), 139–142. http://doi.org/10.1177/0036933013496944
Dingwall, K. M., Delima, J. F., Gent, D., & Batey, R. G. (2015). Hypomagnesaemia and its potential impact on thiamine utilisation in patients with alcohol misuse at the Alice Springs Hospital. Drug and Alcohol Review, 34(3), 323–328. http://doi.org/10.1111/dar.12237
Wijnia, J. W., Wielders, J. P. M., Lips, P., Wiel, A. V. D., Mulder, C. L., & Nieuwenhuis, K. G. A. (2012). Is Vitamin D Deficiency a Confounder in Alcoholic Skeletal Muscle Myopathy? Alcoholism: Clinical and Experimental Research, 37. http://doi.org/10.1111/j.1530-0277.2012.01902.x
Rink, E. B. (1986). Magnesium Deficiency in Alcoholism. Alcoholism: Clinical and Experimental Research, 10(6), 590–594. http://doi.org/10.1111/j.1530-0277.1986.tb05150.x
Harris, R. A., Trudell, J. R., & Mihic, S. J. (2008). Ethanols Molecular Targets. Science Signaling, 1(28). http://doi.org/10.1126/scisignal.128re7
Frazier, T. H., Stocker, A. M., Kershner, N. A., Marsano, L. S., & Mcclain, C. J. (2010). Treatment of alcoholic liver disease. Therapeutic Advances in Gastroenterology, 4(1), 63–81. http://doi.org/10.1177/1756283×10378925
Arteel, G., Marsano, L., Mendez, C., Bentley, F., & Mcclain, C. J. (2003). Advances in alcoholic liver disease. Best Practice & Research Clinical Gastroenterology, 17(4), 625–647. http://doi.org/10.1016/s1521-6918(03)00053-2
Clugston, R. D., & Blaner, W. S. (2012). The Adverse Effects of Alcohol on Vitamin A Metabolism. Nutrients, 4(5), 356–371. http://doi.org/10.3390/nu4050356
Ogunsakin, O., Hottor, T., Mehta, A., Lichtveld, M., & Mccaskill, M. (2016). Chronic Ethanol Exposure Effects on Vitamin D Levels among Subjects with Alcohol Use Disorder. Environmental Health Insights, 10. http://doi.org/10.4137/ehi.s40335
Tardelli, V. S., Lago, M. P. P. D., Silveira, D. X. D., & Fidalgo, T. M. (2017). Vitamin D and alcohol: A review of the current literature. Psychiatry Research, 248, 83–86. http://doi.org/10.1016/j.psychres.2016.10.051
Iber, F. L., Shamszad, M., Miller, P. A., & Jacob, R. (1986). Vitamin K Deficiency in Chronic Alcoholic Males. Alcoholism: Clinical and Experimental Research, 10(6), 679–681. http://doi.org/10.1111/j.1530-0277.1986.tb05167.x