
Low carb and keto are popular dietary paradigms for individuals looking to lose weight and/or improve their health. However, one of the concerns for such individuals is whether or not increasing the amount of saturated fat consumed will increase their LDL cholesterol. Consistent evidence demonstrates that saturated fat increases LDL, but there is not much evidence about how this effect manifests in the context of a low-carb, high-fat diet that restricts carbohydrates to < 5% total energy, as is often the case in well-constructed ketogenic diets.
Does LDL-C Increase On A Low Carb High Fat Or Keto Diet?
Retterstøl et al. (2018) sought to shed light on this question by putting 15 young, healthy adults on a Low Carb High Fat (LCHF) diet for 3 weeks, with the following dietary instructions:
- Follow the guidelines described in Dr. Atkins’ New Diet Revolution aiming to limit carbohydrate intake, and otherwise eat ad libitum.
- The amount of carbohydrates was restricted to <20g/day or <5% of total energy.
- No specific requirements for energy distribution between the intake of protein and fat.
- Participants could eat unlimited quantities of poultry, meat, fish, seafood, eggs and vegetable oils.
- A partial limited intake existed for some food items such as whole-fat cheeses containing carbohydrates and vegetables with low carbohydrate content, such as spinach, sprouts, mushrooms, cucumber and avocado.
- The use of sweeteners such as sucralose, saccharin, cyclamate, acesulfame K, aspartame and erythritol was allowed.
- Due to diet restrictions on carbohydrates, beer, wine and liquor containing carbohydrate alcohol were naturally limited in the LCHF group but there were no restriction on alcohol intake as such.
The 15 participants in the control group to which the LCHF group was compared were instructed to continue with their ordinary diet.
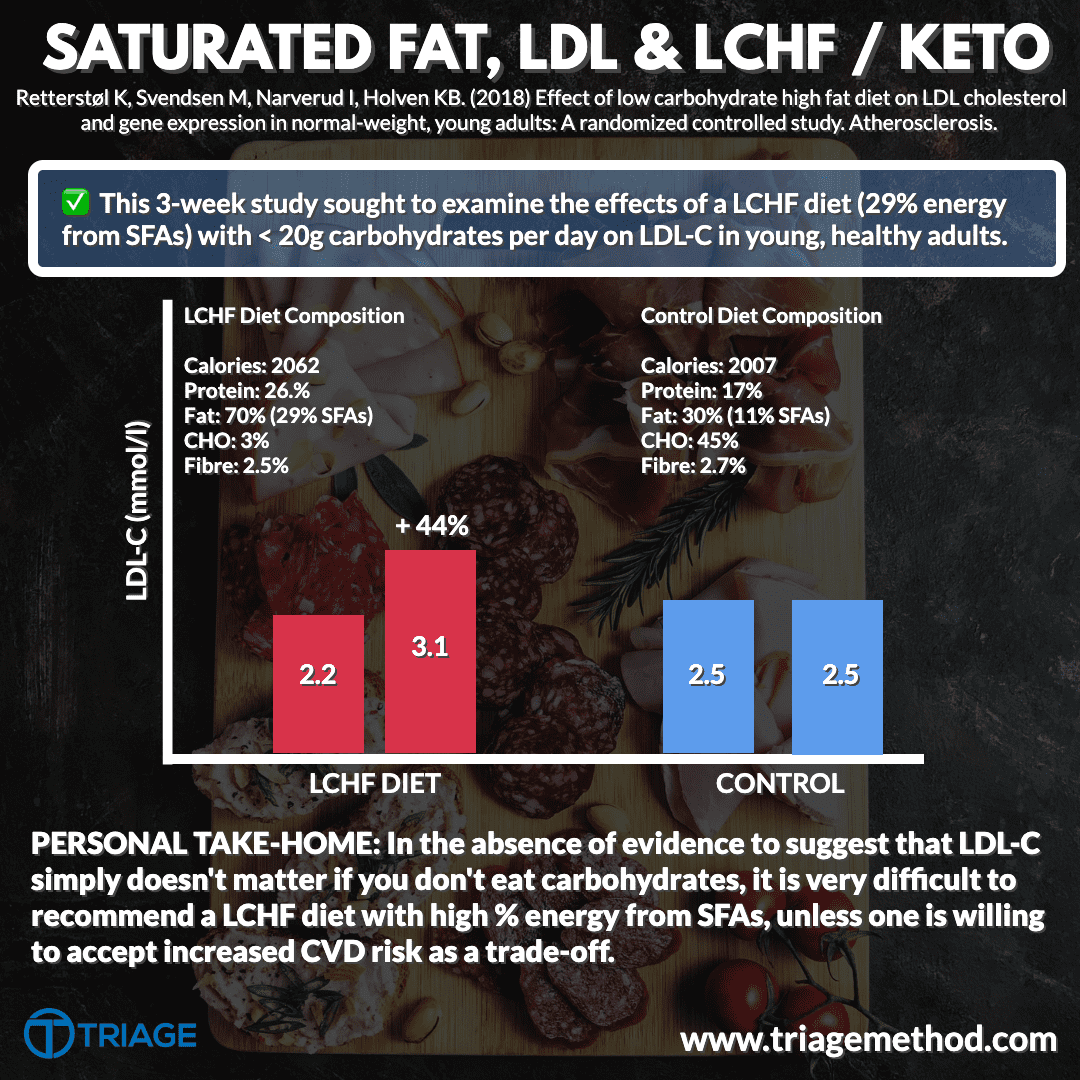
At the end of the 3-week study period, the researchers assessed changes in LDL cholesterol, as well as other important metrics related to cardiovascular risk. Of note, LDL cholesterol increased by 44% in just 3 weeks from 2.2 mmol/l to 3.1 mmol/l in the LCHF group, but stayed the same at 2.5 mmol/l in the control group. The dietary compositions are listed above, and most notably, saturated fat intake was 29% in the LCHF group, 3x the recommended threshold.
Therefore, in the absence of evidence to suggest that elevated LDL-C does not confer cardiovascular risk in those who eat low carbohydrate diets, it is very difficult to ethically recommend this type of diet with high saturated fat as a means of reducing cardiovascular risk.
Putting This In Context
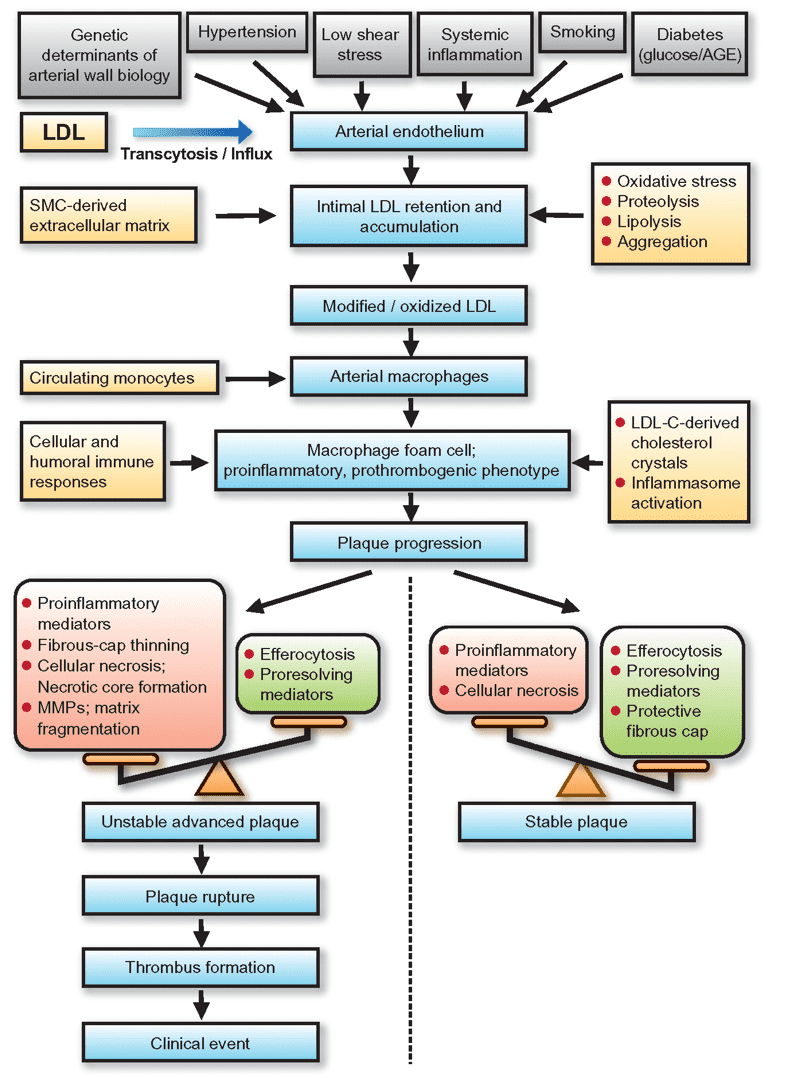
The evidence for supporting LDL-C as a driver of the atherosclerotic process and hence cardiovascular disease is overwhelming (Bóren et al. 2020). Despite this, the acceptance of 1) the role of LDL-C in cardiovascular disease and 2) the detrimental effects of excess saturated fat in the diet have been downplayed or outright denied by many individuals. While many other factors are involved, the body of evidence includes meta-analyses of over 200 prospective cohort studies, Mendelian randomisation, and RCTs consisting of over 2 million participants with over 20 million person-years of follow-up and over 150 000 cardiovascular events, which demonstrates a consistent dose-dependent relationship between the magnitude and duration of LDL-C exposure and risk of atherosclerotic cardiovascular disease (Ference et al. 2017).
Jan Borén, M John Chapman, Ronald M Krauss, Chris J Packard, Jacob F Bentzon, Christoph J Binder, Mat J Daemen, Linda L Demer, Robert A Hegele, Stephen J Nicholls, Børge G Nordestgaard, Gerald F Watts, Eric Bruckert, Sergio Fazio, Brian A Ference, Ian Graham, Jay D Horton, Ulf Landmesser, Ulrich Laufs, Luis Masana, Gerard Pasterkamp, Frederick J Raal, Kausik K Ray, Heribert Schunkert, Marja-Riitta Taskinen, Bart van de Sluis, Olov Wiklund, Lale Tokgozoglu, Alberico L Catapano, Henry N Ginsberg, Low-density lipoproteins cause atherosclerotic cardiovascular disease: pathophysiological, genetic, and therapeutic insights: a consensus statement from the European Atherosclerosis Society Consensus Panel, European Heart Journal, Volume 41, Issue 24, 21 June 2020, Pages 2313–2330, https://doi.org/10.1093/eurheartj/ehz962
Therefore, while a diet that increases LDL-C may confer other health benefits, we cannot conclude that it is universally healthful, nor can we conclude that losing weight, feeling better, or looking good are factors that override the causality of LDL-C in atherosclerotic cardiovascular disease. In the aforementioned study, responses varied profoundly and hence your assessment of cardiovascular risk should not rely solely on average responses to diet, but also on measures taken by your doctor. You may be consuming 15-20% of energy from saturated fat (recommended < 10%) and have LDL-C that is within the healthy range and no other signs of ill health, whereas someone else may be below the 10% threshold and still have elevated LDL-C. Unfortunately, nutrition is not all that counts here.
The good news is that it is not simply the absence of carbohydrates that is driving up LDL. While certain carbohydrate-based foods (whole grains, beans, legumes, and other sources of fibre) can reduce LDL, the replacement of saturated fat with unsaturated fat (especially polyunsaturated fat) appears to be the most potent dietary change for LDL reduction (Mozaffarian et al. 2010; Li et al. 2015; Hooper et al. 2020;). Therefore for someone who just loves a low carbohydrate diet, making some simple swaps to olive oil vs butter, salmon vs fatty steak, more lean meats, less processed meat, a little more fibre, etc. could be enough to avoid these increases in LDL-C while still preserving the other health-promoting effects of the diet.
It doesn’t have to be an either-or between carnivore vs vegan.
We recommend reading the following article if you are interested in learning how to structure a diet.
References & Further Reading
Hooper L, Martin N, Jimoh OF, Kirk C, Foster E, Abdelhamid AS. Reduction in saturated fat intake for cardiovascular disease. Cochrane Database of Systematic Reviews 2020, Issue 5. Art. No.: CD011737. DOI: 10.1002/14651858.CD011737.pub2.
Jan Borén, M John Chapman, Ronald M Krauss, Chris J Packard, Jacob F Bentzon, Christoph J Binder, Mat J Daemen, Linda L Demer, Robert A Hegele, Stephen J Nicholls, Børge G Nordestgaard, Gerald F Watts, Eric Bruckert, Sergio Fazio, Brian A Ference, Ian Graham, Jay D Horton, Ulf Landmesser, Ulrich Laufs, Luis Masana, Gerard Pasterkamp, Frederick J Raal, Kausik K Ray, Heribert Schunkert, Marja-Riitta Taskinen, Bart van de Sluis, Olov Wiklund, Lale Tokgozoglu, Alberico L Catapano, Henry N Ginsberg, Low-density lipoproteins cause atherosclerotic cardiovascular disease: pathophysiological, genetic, and therapeutic insights: a consensus statement from the European Atherosclerosis Society Consensus Panel, European Heart Journal, Volume 41, Issue 24, 21 June 2020, Pages 2313–2330, https://doi.org/10.1093/eurheartj/ehz962
Li, Y., Hruby, A., Bernstein, A. M., Ley, S. H., Wang, D. D., Chiuve, S. E., Sampson, L., Rexrode, K. M., Rimm, E. B., Willett, W. C., & Hu, F. B. (2015). Saturated Fats Compared With Unsaturated Fats and Sources of Carbohydrates in Relation to Risk of Coronary Heart Disease: A Prospective Cohort Study. Journal of the American College of Cardiology, 66(14), 1538–1548. https://doi.org/10.1016/j.jacc.2015.07.055
Mozaffarian, D., Micha, R., & Wallace, S. (2010). Effects on coronary heart disease of increasing polyunsaturated fat in place of saturated fat: a systematic review and meta-analysis of randomized controlled trials. PLoS medicine, 7(3), e1000252. https://doi.org/10.1371/journal.pmed.1000252
Retterstøl K, Svendsen M, Narverud I, Holven KB. Effect of low carbohydrate high fat diet on LDL cholesterol and gene expression in normal-weight, young adults: A randomized controlled study. Atherosclerosis. 2018;279:52-61. doi:10.1016/j.atherosclerosis.2018.10.013