This foundational sleep hygiene overview is the culmination of all the stuff we have been discussing so far in this sleep series. And the purpose is to give you a clear, concise overview of how to get good sleep.
You already know sleep matters. You’ve read the articles, seen the headlines, and heard the podcast episodes. Poor sleep increases your risk of practically every chronic disease, impairs your cognitive function, weakens your immune system, and makes you miserable to be around. Good sleep does the opposite; it’s restorative, protective, energising. You know all this.
And yet here you are, still struggling to get decent sleep most nights. Perhaps you lie awake for an hour before finally drifting off. Perhaps you wake at 3am with your mind racing. Perhaps you sleep a solid eight hours but still wake up feeling like you’ve been hit by a lorry. The knowledge hasn’t translated into better sleep, which means something else is missing.
What’s missing isn’t more information about why sleep matters, it’s a practical, systematic approach to actually improving it. This article is that approach. We’re going to build a complete foundational sleep hygiene system from the ground up, drawing on everything covered in the previous articles in this series. You’ll learn not just what to do, but how to do it, when to do it, and how to troubleshoot when it doesn’t work. More importantly, you’ll learn how to think about sleep improvement so you can adapt these principles to your own life rather than just following a rigid protocol.
Ultimately, sleep hygiene isn’t complicated. The foundations are remarkably straightforward, almost boringly so. Consistent sleep schedule, appropriate light exposure, cool dark room, limited caffeine, etc. None of this is revolutionary. But straightforward doesn’t mean easy, and knowing what to do is very different from actually doing it. The gap between knowledge and implementation is where most people get stuck, and it’s where we’ll spend most of our time in this article.
This isn’t just about optimising metrics or adding years to your life, though those things matter. Better sleep is fundamentally about expanding your capacity to live well. When you sleep properly, you have the energy to pursue what matters to you, the clarity to make good decisions, the emotional regulation to maintain relationships, and the resilience to handle stress. Poor sleep doesn’t just make you tired, it shrinks your world, limits your possibilities, and prevents you from showing up as the person you’re capable of being. Sleep is the foundation upon which you build everything else. So, it makes sense to get your foundational sleep hygiene habits in place.
Table of Contents
- 1 The Philosophy: How to Approach Sleep Improvement
- 2 Assessment: Where Are You Now?
- 3 The Complete Sleep Hygiene Framework: The 10 Foundations
- 3.1 Foundation 1: Track Your Sleep
- 3.2 Foundation 2: Consistent Sleep and Wake Times
- 3.3 Foundation 3: Wind-Down Routine
- 3.4 Foundation 4: Light Exposure Management
- 3.5 Foundation 5: Sleep Environment
- 3.6 Foundation 6: Stimulant Management
- 3.7 Foundation 7: Exercise
- 3.8 Foundation 8: Diet and Nutrition
- 3.9 Foundation 9: Body Weight Management
- 3.10 Foundation 10: Stress Management
- 4 The 80/20: Highest-Yield Sleep Habits
- 5 Your Personalised Sleep Improvement Plan
- 6 Common Obstacles and Solutions
- 6.1 “I Don’t Have Time”
- 6.2 “My Schedule is Irregular (Shift Work, Travel, etc.)”
- 6.3 “My Partner Has Different Sleep Needs”
- 6.4 “I Have Young Children”
- 6.5 “I’ve Tried Everything and Nothing Works”
- 6.6 “I Feel Worse When I Try to Sleep More”
- 6.7 “I’m Anxious About Not Sleeping”
- 6.8 “I Need Caffeine to Function”
- 7 When to Seek Professional Help
- 8 The Long Game: Maintaining Good Sleep
- 9 Foundational Sleep Hygiene Overview
- 10 Author
The Philosophy: How to Approach Sleep Improvement
Before we dive into specific habits and protocols, we need to establish how to think about sleep improvement. Most people approach this the wrong way, which is why they fail despite having access to good information. They try to implement everything at once, expect immediate results, give up when things don’t improve fast enough, or become paralysed by the pursuit of perfect sleep hygiene. Let’s establish some principles that will actually serve you.
Start Where You Are
The first step in improving your sleep is getting honest about where you currently stand. Not where you think you should be, not where you were five years ago, not where your mate with “perfect sleep” supposedly is; where you actually are right now. This requires setting aside any shame or judgement about your current sleep habits and just gathering data.
How much sleep are you actually getting? Not how much you think you’re getting, but actual hours in bed asleep. When do you typically fall asleep? How long does it take you to drift off? Do you wake during the night? How many times? For how long? How do you feel upon waking? Throughout the day? Be specific. Vague assessments like “I don’t sleep well” aren’t useful. You need concrete information about your sleep patterns, your habits, and your problems.
Once you have a clear picture of your current situation, you can identify your biggest problems. This matters because not all sleep issues require the same interventions, and you want to focus your energy on the changes that will actually address your specific problems rather than implementing every possible sleep hygiene recommendation. Someone who can’t fall asleep needs different interventions than someone who can’t stay asleep, and someone who sleeps eight hours but wakes up exhausted has different issues than someone who only sleeps five hours.
The assessment phase isn’t exciting. It doesn’t feel like you are actually making progress, but it’s essential, because you can’t fix what you haven’t properly identified. Spend a week just tracking and observing before you change anything. Note patterns. Look for correlations. Build a clear picture of what’s actually happening rather than operating on assumptions.
Progress Over Perfection
You don’t need perfect sleep hygiene. Let me say that again because it’s important: you don’t need perfect sleep hygiene. You need good enough sleep hygiene, consistently applied. The person who maintains five solid sleep habits every night will get far better sleep than the person who occasionally implements fifteen habits perfectly.
This matters because the pursuit of perfect sleep hygiene often becomes an obstacle to better sleep. People read about every possible esoteric intervention like blackout curtains, blue light glasses, specific supplements, particular foods at particular times, elaborate wind-down routines, mouth tape, weighted blankets, specific pillow arrangements, or sleep trackers analysing every metric, and become overwhelmed. They try to implement everything at once, can’t maintain it, feel like failures, and give up. Or they become so anxious about getting perfect sleep that the anxiety itself prevents them from sleeping well.
Good enough is actually good enough. A consistent bedtime that’s within 30 minutes of your ideal target beats occasionally hitting your exact ideal bedtime. A simple 20-minute wind-down routine you’ll actually do beats an elaborate 90-minute protocol you’ll abandon after three days. Decent curtains that block most light beat the theoretically superior full blackout option you’ll never get around to buying and installing.
Small improvements compound over time, which means consistency beats intensity. Five nights of decent sleep hygiene will serve you better than one night of perfect sleep hygiene followed by six nights of chaos. This is a long game, and the person who can maintain reasonable practices for months and years will always outperform the person who occasionally achieves perfection.
Individual Experimentation
What works brilliantly for one person may do nothing for you, or even make things worse. Sleep hygiene has general principles that apply broadly, but the specific implementation needs to be tailored to your individual biology, psychology, preferences, and constraints. This means you need to be willing to experiment.
Some people notice dramatic improvements from blue light blocking glasses while others see no difference whatsoever. Some people sleep better with the window open, regardless of outside noise, while others need complete silence. Some people find a warm shower before bed helps them drift off easily, while others find it energising and disruptive. Some people need complete darkness to sleep well, while others are fine with a bit of ambient light. You won’t know what works for you until you actually try it.
This requires treating yourself as an experiment rather than just following prescriptions. When you implement a change, give it enough time to assess properly. This usually means at least two to four weeks for most sleep habits. Track what you’re doing and how it affects your sleep. Look for patterns and correlations. Be willing to adjust based on what you discover rather than rigidly adhering to what “should” work according to some article you read.
The goal is to become your own sleep scientist. Develop hypotheses about what might help your specific situation, test them systematically, assess the results honestly, and adjust accordingly. This approach gives you agency and builds genuine understanding rather than just blindly following instructions.
The Positive Feedback Loop
Sleep improvements make other healthy habits easier, which in turn makes sleep easier. This positive feedback loop is one of the most powerful forces in health improvement, but it works in both directions. Poor sleep makes it harder to eat well, exercise consistently, and manage stress, which makes your sleep worse, which makes those other habits even harder, and so the negative spiral continues.
The good news is that once you get some momentum in a positive direction, things get progressively easier. When you start sleeping better, you have more energy to exercise. When you exercise more, you sleep better. When you sleep better, you have better appetite regulation and willpower, making healthy eating easier. When you eat better, you sleep better. When you sleep better, you manage stress more effectively. When you manage stress better, you sleep better. The improvements compound and reinforce each other.
This means your initial efforts might feel disproportionately difficult compared to the results you see. This is because you’re not just implementing new habits, you’re working against the momentum of the negative feedback loop that’s been keeping you stuck. But once you break through and establish some positive momentum, continuing becomes much, much easier. The habits that felt like they required enormous willpower at the start become almost automatic once the positive spiral kicks in.
Be patient through the initial phase. The first few weeks are the hardest because you’re doing the work before you’re seeing the full benefits. But if you can maintain consistency through that difficult early period, the positive feedback loop starts working in your favour and maintaining good sleep hygiene becomes progressively easier.
Systems Over Willpower
If you’re relying on willpower and motivation to maintain good sleep hygiene, you’ve already lost. Willpower feels like it is a finite resource that gets depleted throughout the day, and by the time evening rolls around (precisely when many sleep hygiene habits need to happen!), you feel like you have very little left. Motivation is unreliable, fluctuating based on how you feel, what else is happening in your life, and whether you’re seeing immediate results.
The solution is to build systems and routines that make good sleep hygiene the path of least resistance. This means removing barriers, designing your environment intentionally, and creating structures that don’t depend on moment-to-moment decision-making.
Set alarms for both bedtime and wake time so you’re not relying on noticing the time and choosing to go to bed. Put blue light blocking glasses next to your laptop so you don’t have to remember to find them. If you have one, set your thermostat to automatically lower the temperature in your bedroom at night. Install good curtains so that darkness happens automatically. Keep your phone charger outside your bedroom so you’re not tempted to scroll. Create a consistent wind-down routine so the sequence of activities signals bedtime without requiring active thought.
Environment design matters enormously. If your bedroom is also your office, entertainment centre, and dining room, your brain has no clear signal that this space is for sleep. If your comfortable lounging space is your bed, you’re training yourself to associate your bed with wakefulness. If you keep your phone on your bedside table, you’ll reach for it. If you have to actively decide each night whether to do your wind-down routine or just collapse into bed, you’ll choose collapse most nights.
Build systems that make the good choice automatic and the poor choice require effort. This is how you translate good intentions into consistent behaviour, and consistent behaviour is what actually improves your sleep.
Assessment: Where Are You Now?
Before implementing any changes, you need to understand your current sleep situation. This assessment serves multiple purposes: it identifies your specific problems so you can target your interventions appropriately, it establishes a baseline against which you can measure progress, and it forces you to get honest about your actual sleep rather than operating on assumptions.
Quick Sleep Quality Assessment
Start with these basic questions and answer them honestly based on the past week or two:
On a scale of 1-10, how would you rate your overall sleep quality? Not how much sleep you think you should be getting, not compared to some idealised perfect sleep, but your actual subjective experience of your sleep quality right now.
How many hours do you typically get from the time you fall asleep to the time you wake up? Be honest about actual sleep time, not just time in bed. If you get into bed at 11pm but scroll on your phone until midnight, then lie awake until 12:30am before falling asleep, and wake at 7am, you’re getting 6.5 hours of sleep, not 8 hours.
How consistent is your sleep schedule? Do you go to bed and wake up at roughly the same time every day, including weekends? Or does your schedule vary significantly from day to day?
How long does it typically take you to fall asleep once you’re in bed with the lights off? Five minutes? Thirty minutes? An hour or more? This is called sleep onset latency, and whilst some variation is normal, consistently taking more than 30 minutes to fall asleep suggests a problem.
Do you wake during the night? How often? For how long? Some brief awakenings are normal and you might not even remember them, but if you’re waking multiple times and lying awake for extended periods, that’s relevant information.
How do you feel upon waking? Refreshed and ready to start the day? Groggy but functional after a bit of time? Exhausted and struggling to get out of bed? Do you feel like you could easily fall back asleep?
Do you rely on caffeine to function? Not just “do you drink coffee,” but do you need caffeine to feel awake and alert? Could you function reasonably well without it, or would you be completely useless?
How’s your energy throughout the day? Steady and consistent? Initial morning energy that crashes in the afternoon? Tired all day but wired at night? Do you experience an afternoon slump? How severe is it?
These questions give you a baseline understanding of your sleep quality and help identify patterns. If you’re taking an hour to fall asleep but then sleeping solidly through the night, that’s a different problem than falling asleep quickly but waking multiple times. If you’re getting eight hours in bed but still exhausted, that’s different from only getting five hours. The interventions need to match the problems.
Identifying Your Primary Issues
Based on your assessment, you likely fall into one or more of these categories. Understanding your primary issue helps you prioritise which foundational sleep hygiene habits will give you the biggest return on investment.
Sleep onset issues: You struggle to fall asleep. You’re tired when you get into bed, but the moment your head hits the pillow your mind starts racing or you simply lie there awake. This might mean taking 30 minutes, an hour, or even longer to actually fall asleep.
Sleep maintenance issues: You fall asleep easily enough, but you can’t stay asleep. You wake multiple times during the night, sometimes able to fall back asleep quickly, other times lying awake for extended periods. Or you wake up far earlier than you’d like and can’t get back to sleep.
Poor sleep quality despite adequate time: You’re spending enough time in bed, maybe even eight or nine hours, but you still wake up feeling exhausted. You don’t feel like you slept well, even though you were technically asleep for a reasonable duration.
Daytime sleepiness and fatigue: Regardless of how long you sleep or how “well” you seem to sleep, you’re struggling with excessive daytime sleepiness. You could fall asleep at any moment if you sat still. You’re fighting to stay awake during the day despite seemingly adequate sleep.
Multiple issues: You might have a combination of these problems, which is actually quite common. Perhaps you struggle to fall asleep and then also wake multiple times during the night. Or you fall asleep fine but wake early and can’t get back to sleep, leading to insufficient total sleep time.
Common Sleep Problem Patterns
Beyond just identifying which phase of sleep is problematic, certain patterns emerge that point toward specific underlying issues and, therefore, specific intervention priorities. Recognising your pattern helps you understand what’s driving your sleep problems.
The “Wired and Tired” Pattern: You’re exhausted all day, barely able to function, but the moment you get into bed, you’re suddenly wide awake. Your mind is racing, you feel restless, and sleep seems impossible despite having been desperate for it all day. This pattern is often related to excessive stimulant use, chronic stress, poor light exposure patterns (not enough bright light during the day, too much bright light in the evening), and irregular sleep schedules that have completely confused your circadian rhythm. Primary interventions for this pattern include aggressive caffeine management, stress reduction techniques, proper light exposure timing, and establishing schedule consistency.
The “Racing Mind” Pattern: You’re physically tired when you get into bed, but you simply cannot shut off your thoughts. You’re mentally reviewing the day, planning tomorrow, worrying about problems, having imaginary conversations, or just experiencing a stream of random thoughts that won’t stop. This pattern is often related to high stress, lack of a proper wind-down routine that helps transition your brain from active mode to sleep mode, doing cognitively demanding work late into the evening, or insufficient processing of stress and emotions during waking hours. Primary interventions include establishing a structured wind-down routine, stress management practices throughout the day, keeping a worry journal, and avoiding mentally demanding work in the evening.
The “Can’t Stay Asleep” Pattern: Falling asleep isn’t your problem, and you can actually drift off easily enough. But staying asleep is nearly impossible. You wake multiple times during the night, sometimes for obvious reasons (needing to urinate, too hot or cold, noise) and sometimes for no apparent reason at all. Or you sleep for a few hours and then wake up far earlier than you’d like, unable to get back to sleep. This pattern is often related to environmental issues (room too warm, too much light, noise), alcohol consumption (which helps you fall asleep but disrupts sleep architecture and causes awakenings), excessive caffeine even earlier in the day, high stress and anxiety, or underlying health issues like sleep apnoea. Primary interventions include optimising your sleep environment, eliminating alcohol and reducing caffeine, stress management, and potentially medical evaluation if the problem persists.
The “Never Enough” Pattern: By all accounts you should feel rested. You’re spending eight or even nine hours in bed, you don’t recall waking up much, and you seem to be sleeping. But you wake up feeling like you’ve been hit by a truck. No amount of time in bed seems to be enough. You’re perpetually exhausted despite apparently adequate sleep duration. This pattern often indicates poor actual sleep quality even though you’re technically asleep, which can be caused by sleep apnoea or other sleep disorders, being significantly overweight (which increases sleep apnoea risk and reduces sleep quality), poor sleep environment preventing deep restorative sleep, or inconsistent sleep schedules that never allow your circadian rhythm to properly stabilise. Primary interventions include optimising your sleep environment, weight management if relevant, medical evaluation to rule out sleep disorders, and aggressive schedule consistency.
Identifying your pattern helps you understand not just what’s wrong but why it’s wrong, which points you toward the most relevant interventions rather than just blindly implementing every possible sleep hygiene recommendation.
The Complete Sleep Hygiene Framework: The 10 Foundations
Now we get to the actual habits and practices that constitute solid foundational sleep hygiene. These are the ten core foundations that we use with coaching clients and teach on our sleep coaching course. Not everyone needs to implement all ten, and your specific situation determines your priorities, but these represent the complete framework from which you’ll build your personalised approach.
Foundation 1: Track Your Sleep
What: Systematically monitor your sleep patterns and habits.
Why: You can’t improve what you don’t measure. Tracking serves multiple purposes: it helps you identify specific problems and patterns, it allows you to measure whether your interventions are actually working, it keeps you accountable to your sleep hygiene practices, and it provides objective data rather than subjective impressions that might be unreliable.
How: The simplest approach is keeping a basic sleep diary. Each morning, note what time you got into bed, roughly what time you fell asleep, whether you woke during the night and for how long, what time you woke up, and how you feel upon waking (you can use a simple 1-10 rating). You might also note relevant factors like caffeine intake, alcohol consumption, exercise, stress levels, or anything else that might affect sleep. This takes perhaps five minutes per day.
Alternatively, you can use a wearable device like a fitness watch or sleep tracking ring. These aren’t perfect, and they tend to overestimate sleep duration and aren’t always accurate about sleep stages, but they do provide useful quantitative data about sleep duration, time in bed, and general patterns. The key is not getting obsessively attached to the data. These devices are tools to help you spot patterns and measure general progress, not precision instruments you should worry about optimising.
Time investment: Five minutes per day for manual tracking, essentially nothing if using a wearable you already own.
Priority level: High, especially when you’re first starting to address sleep issues. Once you’ve established good habits and your sleep has stabilised, you can reduce tracking to periodic check-ins rather than daily monitoring.
Critical consideration: Some people become pathologically obsessed with sleep tracking, which actually increases anxiety about sleep and makes it worse. If you find yourself excessively worried about your sleep metrics, lying awake concerned about what your tracker will say, or feeling anxious every morning when you check your data, you need to step back from tracking.
The data is supposed to be helpful, not create additional stress.
Foundation 2: Consistent Sleep and Wake Times
What: Go to bed and wake up at the same time every single day, including weekends.
Why: This is arguably the highest return-on-investment habit you can implement for better sleep. Your circadian rhythm thrives on consistency and predictability. When you maintain the same sleep schedule daily, your body learns when to start preparing for sleep (lowering body temperature, releasing melatonin, reducing cortisol, making you naturally drowsy around your usual bedtime, etc.). Similarly, it knows when to wake you up, often before your alarm even goes off. When your schedule is erratic, your circadian rhythm can’t properly entrain to a pattern, which means your body isn’t actively helping you fall asleep or wake up at appropriate times. You’re working against your biology rather than with it.
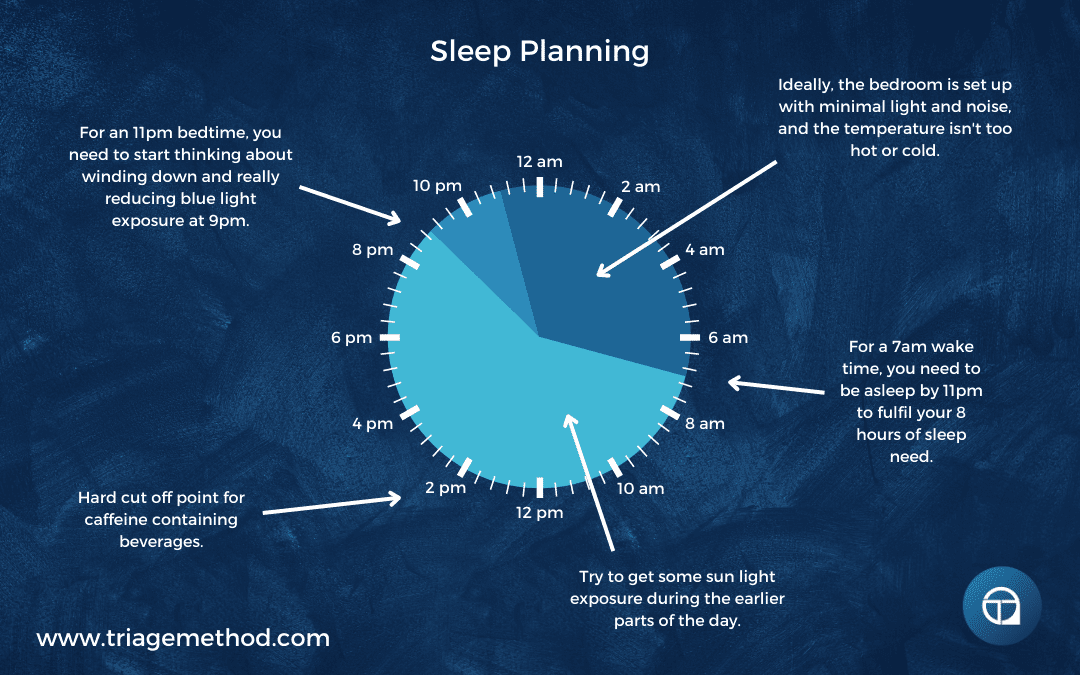
How: The practical implementation is straightforward but requires commitment. First, determine your ideal wake time based on your obligations: work, children, whatever requires you to be up at a certain time. Most people have a hard wake time they can’t negotiate. Then count backward 7.5 to 9 hours (depending on how much sleep you personally need) to determine your bedtime. Add an extra 30 minutes to account for the time it takes to actually fall asleep. This is when you need to be in bed, lights off, attempting sleep.
Set a non-negotiable alarm for your wake time. Set a reminder alarm for your bedtime, perhaps 30 minutes before, so you can start your wind-down routine. Then stick to these times every single day. Not just Monday through Friday. Every day. Weekends included. This consistency is what allows your circadian rhythm to stabilise.
Time investment: This isn’t about time investment; it’s about consistency and planning. The execution is simply going to bed and waking up at set times.
Priority level: Critical. If you’re only going to implement one sleep hygiene habit, this should be it.
Common obstacles: The biggest obstacle is social pressure and lifestyle preferences. People want to stay up late on weekends, go out with friends, and sleep in on Sunday mornings. And yes, maintaining a consistent sleep schedule does require saying no to some things or planning around your sleep needs. This is the fun part where you get to decide whether the short-term pleasure of staying up late or sleeping in is worth the ongoing cost of poor sleep. Most people haven’t made this choice consciously; they’ve just defaulted into patterns that don’t serve them. But you must accept that you’re not a victim of your schedule, you’re choosing it, even if it doesn’t feel like a choice.
Foundation 3: Wind-Down Routine
What: A consistent pre-sleep protocol lasting 30-90 minutes that signals to your body and mind that sleep is approaching.
Why: You can’t go from full cognitive engagement directly to sleep. Your brain and body need time to transition from the stimulation and demands of waking life into a state conducive to sleep. A wind-down routine serves multiple purposes: it reduces psychological and physiological arousal, it provides a clear boundary between waking activities and sleep, it becomes a Pavlovian cue that signals sleep is imminent, and it gives you dedicated time to process the day rather than lying in bed with thoughts racing.
How: Choose 2-5 calming activities and do them in roughly the same order every night. The specific activities matter less than consistency and the overall effect of reducing arousal. Here are some effective options:
A warm shower or bath 30-60 minutes before bed. While you need a lower body temperature to fall asleep, a warm shower causes your body to subsequently cool itself down, which can facilitate sleep onset. The warm water is also relaxing in itself.
Deep, slow breathing exercises. Five to ten minutes of deliberate slow breathing (perhaps box breathing (4 seconds in, 4 seconds hold, 4 seconds out, 4 seconds hold) or simply slow diaphragmatic breathing) can dramatically reduce nervous system activation and create a sense of calm.
Meditation or progressive muscle relaxation. Even brief meditation practices can help settle the mind and reduce the mental chatter that prevents sleep.
Light stretching or foam rolling. Gentle movement and manual therapy can release physical tension and help the body relax.
Journalling. Writing down your thoughts, worries, plans for tomorrow, or things you’re grateful for can help clear your head and reduce the likelihood of lying in bed ruminating. This doesn’t need to be elaborate, and a few minutes with pen and paper is sufficient.
Reading a physical book (ideally not on a screen). Reading is a classic pre-bed activity that many people find naturally induces drowsiness. Physical books are preferable to screens for reasons we’ll discuss in the light exposure section.
Aromatherapy. Some people find scents like lavender helpful for relaxation. Diffusers or pillow sprays are safer options than candles, which present a fire risk if you fall asleep.
The activities you choose should be genuinely relaxing to you personally, not just things you think you should find relaxing. If meditation makes you anxious because you can’t stop your thoughts, it’s not the right choice for you. If reading gets you so engaged you can’t put the book down, choose something else. Experiment to find what actually helps you unwind.
Equally important is what you avoid during wind-down time. This is not the time for work emails, social media scrolling, intense television shows, arguments with your partner, planning complex projects, or anything that increases stress or mental stimulation.
Time investment: 30-90 minutes before your actual bedtime.
Priority level: High, particularly for people with racing mind patterns or difficulty falling asleep.
Common obstacle: People feel they don’t have time for a wind-down routine, which is almost always a prioritisation issue rather than an actual time constraint. If you’re spending the two hours before bed scrolling social media or watching television anyway, you have the time; you’re just not using it intentionally.
Foundation 4: Light Exposure Management
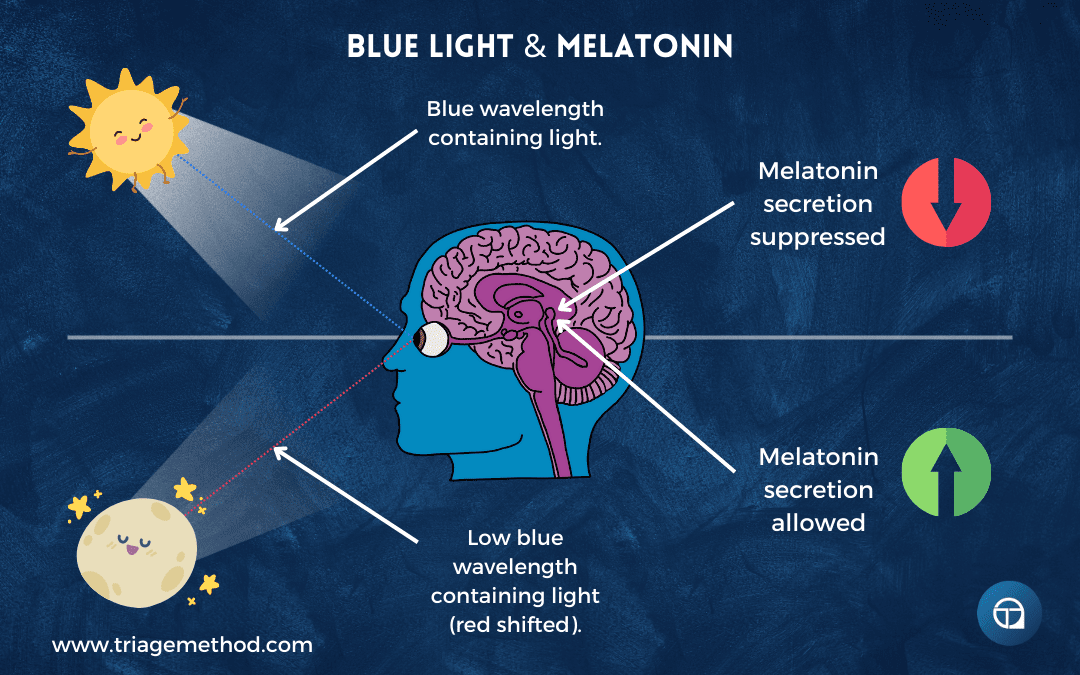
What: Bright light exposure during the day, particularly in the morning, and reduced light exposure in the evening, particularly blue wavelengths.
Why: Light is the primary environmental cue that sets your circadian rhythm. Your body uses light levels to determine whether it should be in daytime mode (alert, energised, suppressing melatonin) or nighttime mode (calm, drowsy, producing melatonin). When you get bright light in the morning, you’re giving your circadian system a clear signal that it’s time to be awake, which then sets in motion a cascade of physiological changes that will make you naturally drowsy at the appropriate time that evening. When you’re exposed to bright light, particularly blue wavelengths, in the evening, you’re sending a confusing signal that it’s still daytime, which suppresses melatonin production and makes it difficult to fall asleep.
The timing and quality of your light exposure throughout the day might be the single most powerful lever you have for regulating your sleep-wake cycle, yet it’s one that most people completely ignore.
How – Morning Light: Get outside within 30-60 minutes of waking and spend at least 10-30 minutes in natural daylight. This doesn’t mean you need to stare directly at the sun, just be outside where your eyes are exposed to bright natural light. Even on cloudy days, outdoor light is significantly brighter than indoor lighting and provides the signal your circadian system needs. If you can combine this with other activities like morning coffee on the porch/balcony, a short walk, or reading outside, it’s easier to maintain consistency.
If getting outside is genuinely impossible due to your circumstances, you can use a light therapy box (often called a SAD lamp) designed to provide bright light therapy. Position it at eye level about 40-60cm away whilst you’re having breakfast or getting ready, and use it for 20-30 minutes. This isn’t quite as effective as natural sunlight, but it’s vastly better than typical indoor lighting.
The key is consistency. Every single day, including weekends and days you don’t have to get up early for work. This is how you train your circadian rhythm to know when morning is.
How – Evening Light: In the 2-3 hours before bed, you want to significantly reduce your light exposure, particularly blue wavelengths, which are most effective at suppressing melatonin. This means several things:
Dim your lights. Instead of using bright overhead lights in the evening, switch to lamps with warm-toned bulbs. You don’t need to be sitting in near-darkness, but the lighting should be noticeably dimmer than during the day.
Reduce screen time, or at the very least manage it properly. Screens emit substantial blue light. If you’re going to use screens in the evening, and realistically most people will, install software like f.lux that automatically reduces blue wavelengths based on the time of day, use your device’s night mode, or wear blue light blocking glasses. The glasses option is often most practical because it works regardless of what device you’re using.
Avoid bright bathrooms. If you need to use the bathroom during your wind-down routine, either keep the lights off (use a small night light if needed) or have dimmer switches installed so you’re not blasting yourself with bright overhead lighting.
Consider blackout conditions. As you get closer to actual bedtime, you want darkness to be increasing. Some people benefit from very dim red or amber lighting in the final hour before sleep, as these wavelengths don’t suppress melatonin.
Time investment: 10-30 minutes of morning light exposure, plus evening behaviour changes.
Priority level: Critical. This is one of the most powerful interventions available, and it’s essentially free.
Common obstacles: People dismiss this as too simple to matter, or they struggle to consistently get morning light because it requires actually going outside rather than just rushing from bed to car to office. Evening light management conflicts with modern life; screens, bright indoor lighting, and late-night activities all work against you. But these obstacles are largely about choice. You can choose to go outside in the morning. You can choose to dim your lights in the evening. The question is whether you’re willing to prioritise sleep over convenience.

Foundation 5: Sleep Environment
What: A bedroom optimised for sleep; cool, dark, quiet, and comfortable.
Why: Your sleep environment either supports or sabotages your physiological sleep processes. Core body temperature needs to drop to initiate sleep, which is difficult if your room is too warm. Darkness is required for proper melatonin production. Noise can prevent you from falling asleep or cause micro-awakenings that fragment your sleep even if you don’t consciously remember waking. Discomfort from a poor mattress or inappropriate bedding prevents deep, restorative sleep. You can have perfect sleep hygiene habits, but still sleep poorly if your environment is working against you.
How – Temperature: For most people, the ideal bedroom temperature is between 15-19°C (60-67°F), perhaps slightly cooler than feels comfortable when you’re awake and dressed. You want the room cool enough that you’re comfortable under covers, but not so cold you’re shivering. This takes some experimentation, and there will likely need to be a compromise if you share a bed with someone whose temperature preferences differ from yours.
You can adjust temperature through several methods: thermostat settings (some thermostats allow you to automatically lower temperature at night), fans for air circulation and cooling, appropriate bedding for the season (lighter covers in summer, warmer in winter), amount of clothing you wear to bed, and in some cases, mattress cooling systems or cooling pillows, though these are more expensive options.
Some people find that allowing the house to gradually cool down during their wind-down period helps trigger drowsiness as the falling temperature parallels their own dropping core temperature and creates an instinctive desire to get under warm covers.
How – Darkness: Your bedroom should be dark enough that you can’t see your hand in front of your face. Light exposure during sleep suppresses melatonin and can cause awakenings or prevent you from achieving deep sleep. This is particularly important in summer when sunrise is early or if you live in an area with substantial light pollution or street lights.
Blackout curtains or blinds are the most effective solution. They completely block external light and allow you to control darkness regardless of the time of year or outside conditions. If blackout curtains aren’t feasible (rental property, cost, aesthetic objections from a partner), a sleep mask can work, though it can slip off during the night, and some people find them uncomfortable.
You also want to eliminate light sources within the bedroom. Cover or remove devices with LED lights (alarm clocks, smoke detectors, chargers). If you need to check the time during the night, use a clock with a dim red display rather than bright blue or green. Don’t leave your phone face-up on the bedside table where notifications will light up the room.
How – Noise: Ideally, your bedroom should be quiet, without disruptive sounds from traffic, neighbours, household members, or pets. In practice, this isn’t always achievable, particularly if you live in a flat, near busy roads, or in areas with significant noise pollution.
If you can control the noise, do so. Close windows if outside noise is significant (though this may conflict with temperature or air quality needs). Have conversations with household members about noise levels during your sleep time. Move pets out of the bedroom if they’re disruptive.
If you can’t control external noise, you have two main options: earplugs or white noise. Good quality earplugs can reduce noise substantially, though some people find them uncomfortable or anxiety-provoking (worry about not hearing alarms or emergencies). White noise machines, fans, or white noise apps create a consistent ambient sound that masks irregular noises and prevents them from being as disruptive. Many people find white noise actually improves their sleep even in the absence of problematic external noise.
How – Air Quality: Good air circulation and appropriate humidity levels matter for sleep quality. Stale air, excessive carbon dioxide buildup, and poor humidity can all reduce sleep quality even if you’re not consciously aware of it.
Opening a window (even slightly) helps ensure fresh air circulation and prevents CO2 buildup, particularly in small bedrooms. This obviously conflicts with noise and temperature control in some situations, so you’ll need to find the right balance for your circumstances. If you can’t have windows open, ensure good air circulation through other means. Some people benefit from air purifiers, particularly if they have allergies or live in areas with poor air quality. Humidifiers or dehumidifiers can help if your environment is too dry or too humid, both of which can disrupt sleep.
How – Comfort: Your mattress, pillows, and bedding should support comfortable sleep for your body. This is highly individual, and some people need firm mattresses, while others need soft, some need multiple pillows, while others need one or none, some need heavy blankets, while others prefer light covers.
If you frequently wake with aches and pains, or if you sleep better in other locations than your own bed, your sleeping setup likely needs adjustment. You don’t necessarily need to spend thousands on a new mattress, but you should be willing to invest reasonable amounts in the place you spend a third of your life. Experiment with different pillow arrangements, consider whether your mattress is too firm or too soft, and try different bedding weights.
Some people benefit from weighted blankets, which can create a sense of security and reduce anxiety. Others find them restrictive. Some people need separate blankets from their partner to avoid cover-stealing conflicts. Some people need complete separation of the sleeping surface (separate mattresses) to avoid being disturbed by a restless partner.
Time investment: One-time setup with ongoing minor adjustments.
Priority level: High. Environmental factors have a substantial impact on sleep quality.
Critical consideration: You spend roughly a third of your life sleeping. Investing time and money into optimising your sleep environment isn’t frivolous; it’s one of the highest-return investments you can make in your health and quality of life.
Foundation 6: Stimulant Management
What: Limiting caffeine intake and establishing a hard cutoff time for consumption, ideally 8-12 hours before bed.
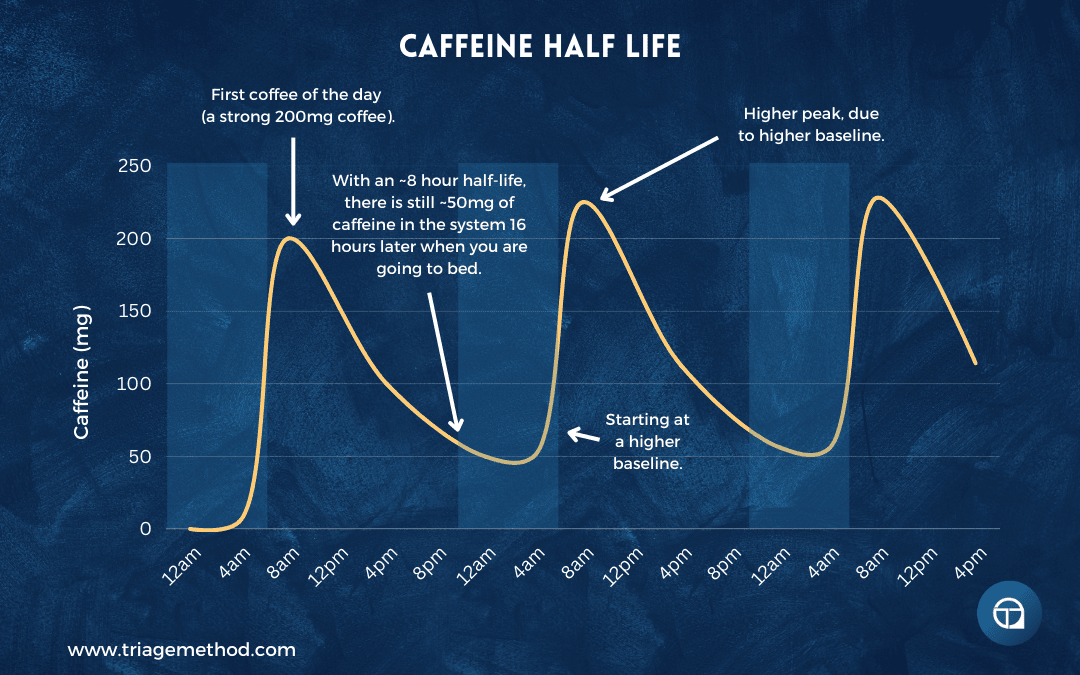
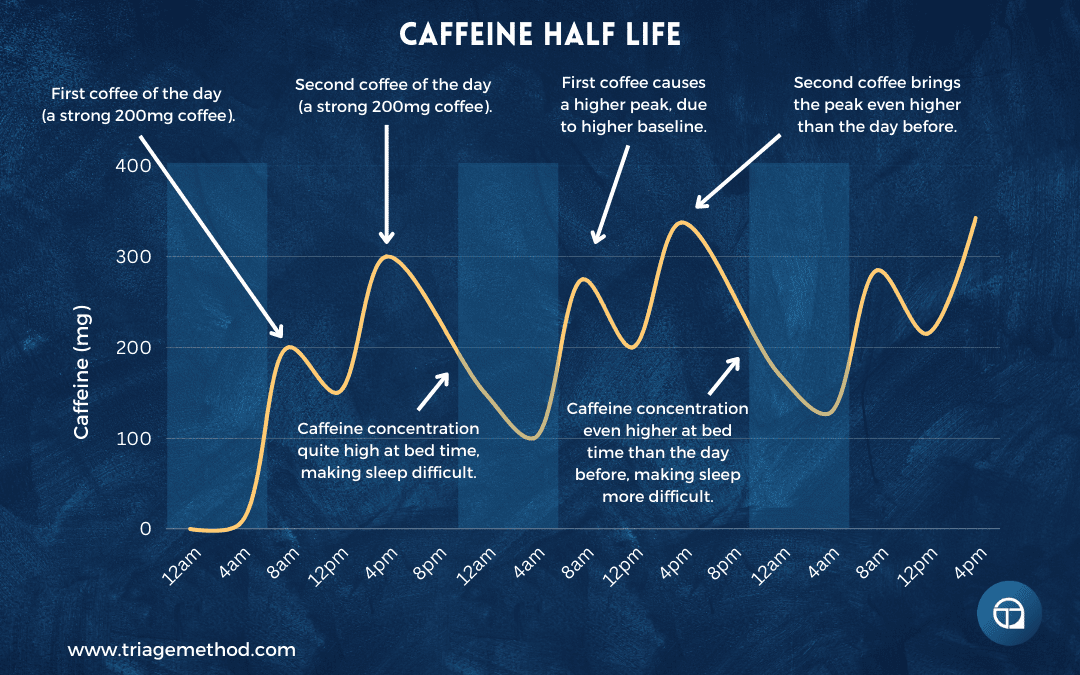
Why: Caffeine is an adenosine antagonist, which means it blocks the accumulation of sleep pressure. Even if you don’t feel wired from caffeine, it’s still interfering with your sleep drive and disrupting your sleep architecture. Research shows that caffeine consumed even six hours before bed significantly disrupts sleep, reducing total sleep time and sleep efficiency. The problem is that caffeine’s half-life is 3-5 hours (highly variable between individuals), meaning that even moderate amounts consumed in the afternoon are still present at substantial levels when you’re trying to sleep.
The other issue is tolerance and dependence. Many people are stuck in a vicious cycle: poor sleep leads to excessive caffeine consumption to function during the day, which then interferes with sleep that night, leading to more caffeine the next day, and so on. Breaking this cycle requires temporarily accepting reduced daytime function whilst you reduce caffeine and improve sleep, but the long-term payoff is not needing to rely on stimulants to feel human.
How: First, audit your actual caffeine intake. Track every source of caffeine for several days: coffee, tea, soft drinks, energy drinks, pre-workout supplements, chocolate, and certain medications. You might be surprised by the total amount. A standard cup of coffee contains roughly 90mg (though this varies substantially with size and brewing method), tea contains 30-50mg, a can of cola contains 35-50mg, and energy drinks can contain 150mg or more per can.
Then establish a hard cutoff time, ideally 12 hours before bed, but at a minimum 8 hours before bed. If you go to bed at 10pm, your last caffeine should be no later than 10am (ideally) or 2pm (at the very latest). This isn’t negotiable; it’s a firm boundary. Set reminders if needed. After your cutoff time, switch to decaffeinated options.
You may also need to reduce your total daily caffeine intake, particularly if you’re consuming more than 400mg per day (the upper limit most health authorities consider reasonably safe). Reduce gradually (something like cutting 25-50mg per day each week) to avoid withdrawal headaches and fatigue. Within 2-4 weeks, your sleep should noticeably improve, and you’ll likely find you actually need less caffeine to function.
Remember that caffeine is hidden in many products beyond just coffee. Tea contains substantial caffeine, despite what people think; a strong cup of black tea can have as much caffeine as a weak coffee. Soft drinks, particularly colas and many other fizzy drinks, contain caffeine. Pre-workout supplements are often loaded with caffeine. Some pain medications contain caffeine. Check the labels.
Time investment: This is purely a behaviour change, and there is no time investment beyond the discipline to stop consuming caffeine after your cutoff time.
Priority level: Critical, especially if you’re a heavy caffeine user or if you consume caffeine in the afternoon or evening.
Common obstacles: The biggest obstacle is that reducing caffeine makes you feel worse before you feel better. When you cut back, you may experience withdrawal symptoms like headaches, fatigue, and/or irritability, and reduced function for a week or two. This is temporary, but it’s unpleasant, and many people give up during this period and return to high caffeine consumption. The other obstacle is social and habitual. If your afternoon routine involves meeting a friend for coffee, or if you habitually have a cup of tea after dinner, changing this feels like a sacrifice. But again, this is about choice. You’re choosing between the short-term comfort of your caffeine habit and the long-term benefit of better sleep.
Foundation 7: Exercise
What: Regular physical activity, preferably 30-90 minutes most days of the week, completed at least 2-3 hours before bed.
Why: Exercise is one of the most robust interventions for improving sleep. It increases sleep pressure (your drive to sleep), improves sleep quality and efficiency, reduces the time it takes to fall asleep, increases time spent in deep sleep, reduces symptoms of sleep disorders like apnoea and restless legs, and helps regulate your circadian rhythm, particularly if done outdoors in daylight. Exercise also helps manage stress, anxiety, and depression, all of which interfere with sleep. The relationship is bidirectional, as exercise improves sleep, and good sleep improves exercise performance and recovery, creating a positive feedback loop.
How: You don’t need anything fancy or complicated. Any form of movement counts. Walking, running, cycling, swimming, strength training, team sports, dancing, yoga, etc., all of it helps. The key is consistency and accumulating enough total activity.
Aim for at least 30 minutes most days, though 60-90 minutes provides additional benefits. Mix both cardiovascular exercise and some form of resistance training if possible, as both have independent benefits for sleep. Higher intensity exercise tends to have stronger effects on sleep than very light activity, but light activity is vastly better than nothing.
Timing matters somewhat. Exercise increases core body temperature, heart rate, and sympathetic nervous system activation, all of which can interfere with sleep if done too close to bedtime. For most people, finishing exercise at least 2-3 hours before bed is ideal. Morning or afternoon exercise is generally better than evening exercise for sleep purposes, though this varies individually, and evening exercise is still better than no exercise.
There’s an additional benefit to exercising outdoors, particularly in morning daylight, as you get both the exercise benefits and the light exposure benefits simultaneously.
Time investment: 30-90 minutes per day.
Priority level: High. Exercise improves essentially every aspect of health, sleep being just one of many benefits.
Common obstacles: Time is the most commonly cited barrier, though it’s often more about prioritisation than actual time scarcity. Pain or injury can legitimately limit exercise options, though there’s almost always some form of movement that’s accessible; even chair exercises or gentle walking can help. Initial discomfort when starting exercise can discourage people, but this improves rapidly with consistency. Some people find exercise interferes with their sleep if done too close to bedtime, which is easily solved by exercising earlier in the day.
Critical consideration: Exercise helps prevent or manage pain, which is important because pain is a major sleep disruptor. Even if you’re not currently experiencing pain that affects sleep, building a robust, resilient body through exercise reduces your likelihood of developing pain that interferes with sleep in the future.
Foundation 8: Diet and Nutrition
What: A balanced, whole-food diet with appropriate meal timing and specific attention to foods and substances that can disrupt sleep.
Why: Your diet affects sleep through multiple mechanisms. Certain nutrients are required for neurotransmitter synthesis involved in sleep regulation. Blood sugar fluctuations affect cortisol and can cause awakenings. Digestive processes can interfere with sleep if you eat too close to bedtime. Specific foods and drinks (particularly alcohol) directly disrupt sleep architecture. Overall diet quality affects inflammation, gut health, and metabolic function, all of which influence sleep.
How – General Diet Quality: The foundation is eating a generally well-balanced diet built primarily on whole foods: adequate protein (roughly 1.6-2.2g per kg of body weight daily), plenty of fruits and vegetables (ideally aim for 8-12 servings daily for micronutrient sufficiency), appropriate amounts of healthy fats, and sufficient carbohydrates without over-restriction. Avoid extreme dietary approaches that eliminate entire macronutrient categories, as low-carb, low-fat, and low-protein diets all have documented negative effects on sleep quality for most people.
How – Meal Timing: Leave at least 2-3 hours between your last meal and bedtime. Eating too close to bedtime keeps your digestive system active when it should be winding down, raises your core body temperature (which opposes the temperature drop needed for sleep), and can cause reflux or discomfort that interferes with sleep. You don’t want to go to bed hungry, that can also disrupt sleep, but you want to finish eating with sufficient time for initial digestion to complete.
Some individuals find that having a larger portion of their daily carbohydrate intake at dinner helps them sleep, though this isn’t universal. You will need to experiment with this to figure out what works for you; try having a well-balanced dinner with adequate carbohydrates and see if it helps your sleep compared to a lower-carb evening meal.
How – Hydration Timing: Stay well-hydrated throughout the day, but taper off fluid intake in the evening. Drinking large amounts of water close to bedtime often results in waking during the night to urinate, which fragments your sleep. Ensure you’re adequately hydrated by the evening, then reduce intake in the last 2-3 hours before bed.
How – Alcohol: Alcohol is one of the most problematic substances for sleep, despite people commonly believing it helps them sleep. Alcohol does help you fall asleep faster (it’s a sedative), but it severely disrupts sleep architecture. It suppresses REM sleep in the first half of the night, causes rebound awakenings in the second half, increases sleep apnoea and snoring, and prevents restorative deep sleep. You might be unconscious for eight hours after drinking, but you’re not getting eight hours of quality sleep.
If you drink alcohol, avoid it in the 4-6 hours before bed at minimum. Better still, reduce overall alcohol consumption or eliminate it entirely if sleep is a priority. Many people report dramatic sleep improvements after eliminating alcohol, even if they were only having a drink or two in the evening.
Time investment: Meal planning and timing, plus the time to prepare nutritious meals.
Priority level: Medium-high. Diet quality matters for sleep, though it’s perhaps less immediately impactful than schedule consistency or light exposure.
Common obstacles: The modern food environment makes healthy eating challenging. Convenience often conflicts with food quality. Social situations revolve around food and alcohol. Time and skill required for meal preparation. The cost of healthy food in some areas. All legitimate obstacles, but again, ultimately about prioritisation and choice. These systemic issues are not going to be fixed by you not tackling what is within your control. Do what you can, where you can.
Foundation 9: Body Weight Management
What: Achieving and maintaining a healthy body weight, particularly if you’re significantly overweight or obese.
Why: Excess body weight, particularly when carried around the neck, chest, abdomen, and upper back, increases the risk of sleep apnoea (a condition where breathing becomes shallow or stops repeatedly during sleep). Sleep apnoea prevents restorative sleep and leaves people exhausted despite spending adequate time in bed. Even without clinical sleep apnoea, excess weight is associated with poorer sleep quality, more frequent awakenings, and less time in deep sleep stages.
Interestingly, very high muscle mass can also contribute to sleep issues for the same mechanical reasons; heavily muscled individuals, particularly enhanced bodybuilders, often develop sleep apnoea. Most people reading this aren’t in that category, but it’s worth noting that the issue is total mass on the upper body affecting airways, not just body fat.
How: If you’re significantly overweight, gradual fat loss through the combination of appropriate dietary changes and increased physical activity will likely improve your sleep. This isn’t quick (sustainable fat loss occurs at perhaps 0.5-1% per week), but the sleep benefits begin accumulating as you lose weight, not just after reaching your goal weight.
This foundation integrates with Foundations 7 and 8 (exercise and nutrition). If you address those properly, weight management often follows naturally for most people. The specific strategies for fat loss are beyond the scope of this sleep article, but the basic principle is creating a sustainable caloric deficit through some combination of eating less and moving more, while maintaining adequate protein intake and resistance training to preserve muscle mass.
If you suspect you might have sleep apnoea (loud snoring, gasping or choking during sleep, observed breathing pauses, excessive daytime sleepiness despite adequate time in bed), medical evaluation is critical. Don’t just assume weight loss will solve it; actually get assessed by a doctor and potentially do a sleep study. Weight loss helps substantially, but you may also need CPAP therapy in the interim.
Time investment: Long-term; months to years depending on how much weight you need to lose. Not a quick fix, but a fundamental change that improves not just sleep but overall health.
Priority level: High if weight is a significant issue. Lower priority if you’re already at a healthy weight.
Common obstacles: The same obstacles that make weight management difficult for many reasons: food environment, social pressures, emotional eating, metabolic adaptations, time requirements for meal prep and exercise, and potentially underlying medical or psychological issues. The vicious cycle is particularly pronounced here: poor sleep makes healthy eating and consistent exercise more difficult, which prevents weight loss, which perpetuates poor sleep.
Foundation 10: Stress Management
What: Daily practices that reduce psychological stress and anxiety, helping manage the mind’s response to life’s demands.
Why: Stress is perhaps the single biggest sleep disruptor. When you’re stressed, your body maintains higher cortisol levels, your sympathetic nervous system stays activated, your mind races with worries and rumination, and you struggle to achieve the relaxed state necessary for sleep. Even if you do fall asleep, stress can cause nighttime awakenings and prevent deep restorative sleep. Chronic stress creates a vicious cycle where stress disrupts sleep, poor sleep reduces stress resilience, leading to more stress and worse sleep.
And ultimately, stress management isn’t just important for falling asleep, it’s important for the entire day. If you spend all day in a high-stress state, you can’t expect to flip a switch and be calm at bedtime. You need to manage stress throughout the day so you’re not arriving at bedtime wound up like a spring.
How: Stress management is highly individual, and what works depends on your stress triggers, personality, and circumstances. Here are effective approaches:
Meditation and mindfulness practices: Even 10-15 minutes of daily meditation helps train your mind to observe thoughts without getting caught up in them, reduces overall arousal, and improves your ability to shift into relaxed states. Apps like Headspace or Calm can provide structure if you’re new to meditation.
Breathing exercises: Simple breathwork practices like box breathing, 4-7-8 breathing, or just slow diaphragmatic breathing, all rapidly calm the nervous system and can be done anywhere, anytime you notice stress rising. Particularly valuable as part of your wind-down routine, but also useful throughout the day.
Journalling: Regular writing helps process emotions, reduce rumination, solve problems, and get worries out of your head and onto paper. Particularly useful to do in the evening as part of a wind-down, or whenever you’re feeling overwhelmed.
Physical activity: We’ve already discussed exercise for sleep, but it’s worth emphasising its stress management benefits. Even a 10-minute walk can substantially reduce stress levels.
Time boundaries and saying no: Much stress comes from overcommitment and poor boundaries. Learning to say no, setting limits on work hours, and protecting time for rest and recovery reduces stress more effectively than any relaxation technique. This requires viewing your time and energy as finite resources you must manage carefully, rather than unlimited commodities to be exploited.
Social connection: Strong relationships and regular social interaction buffer against stress. Isolation increases stress and anxiety. Make time for meaningful connection with friends and family.
Professional help: If stress is severe or chronic, particularly if accompanied by anxiety or depression, working with a therapist can be immensely valuable. Cognitive behavioural therapy, acceptance and commitment therapy, and other evidence-based approaches teach concrete skills for managing stress and anxiety.
Worry window: If you find yourself ruminating in bed, try implementing a “worry window”. This is a designated 15-20 minute period earlier in the evening specifically for worrying and problem-solving. Write down your concerns, potential solutions, and action items. Then, when worries arise at bedtime, remind yourself you’ve already addressed them during your worry window and they can wait until tomorrow’s session.
Time investment: 10-30 minutes per day for structured practices, plus the time saved by better boundaries.
Priority level: Critical if stress levels are high. Medium priority if stress is well-managed.
Common obstacles: Stress management often feels like something you don’t have time for precisely when you need it most. The busier and more stressed you are, the more you need these practices, yet that’s when they’re easiest to skip. You also can’t just “try” meditation for a few days and expect transformation, as these practices work through consistent application over weeks and months. Many people also resist seeking professional help due to stigma or cost, even when they clearly need it.
The 80/20: Highest-Yield Sleep Habits
If implementing all ten foundations feels overwhelming, you can start with just five habits that deliver roughly 80% of the results for most people. These are the absolute core practices that have the highest return on investment.
1. Consistent Sleep and Wake Times
Same bedtime and wake time every single day, including weekends. Set alarms for both. Work backwards from your required wake time to determine your bedtime, allowing 8 hours in bed (for approximately 7-7.5 hours of actual sleep). This is the single most powerful habit for entraining your circadian rhythm and making everything else easier.
Quick implementation: Tonight, right now, decide your sleep schedule. Set your wake alarm and a bedtime reminder. Tomorrow morning, regardless of how you slept, wake at your set time and get light exposure immediately. Tomorrow night, go to bed at your set time. Repeat every single day.
2. Morning Light Exposure
Get outside within 30-60 minutes of waking for 10-30 minutes of natural daylight exposure. Every single day. This sets your circadian clock, suppresses morning melatonin so you feel alert, and ensures proper melatonin production in the evening when you actually want to sleep.
Quick implementation: Take your morning coffee outside. Go for a brief walk. Sit at your doorstep. Open the curtains and stand by the window if you absolutely can’t get outside. Just get light in your eyes early.
3. Evening Light Reduction
Dim your lights 2-3 hours before bed. Reduce screen time or use blue light blocking glasses and night mode. Avoid bright overhead lights. Use warm, dim lamps. Allow your environment to darken gradually as you approach bedtime.
Quick implementation: Install f.lux on your computer tonight. Enable night mode on your phone. Buy blue light blocking glasses (inexpensive and available everywhere). Switch to lamps instead of overhead lights after dinner.
4. Caffeine Cutoff
No caffeine after 12-2pm depending on your bedtime. Set a hard cutoff time and stick to it religiously. Switch to decaf options after your cutoff. If you’re currently having caffeine late in the day, this single change can dramatically improve your sleep.
Quick implementation: Set a phone reminder for your caffeine cutoff time (12pm is ideal, 2pm at the very latest). When it goes off, no more caffeine for the day. Switch to decaf coffee, herbal tea, or water.
5. Cool, Dark, Quiet Bedroom
Room temperature between 15-19°C (60-67°F). Complete darkness—blackout curtains or sleep mask. Minimal noise—earplugs or white noise if needed. These environmental factors are essential for quality sleep regardless of your habits.
Quick implementation: Lower your bedroom thermostat tonight. Order blackout curtains this week. Download a white noise app or move a fan into your bedroom. Cover or remove electronics with bright LED lights.
These five habits alone will dramatically improve most people’s sleep within a few weeks. They address the core mechanisms (circadian entrainment, sleep drive, environmental optimisation) without requiring elaborate protocols or major lifestyle overhaul.
Your Personalised Sleep Improvement Plan
Now that you understand the foundations, you need to build a personalised plan based on your specific situation and primary issues. Not everyone needs to implement everything, and trying to change everything at once usually leads to failure. Here’s how to build your plan systematically.
Step 1: Prioritise Based on Your Situation
High priority for everyone: Regardless of your specific sleep issues, these habits have universal benefits and should be your starting point:
- Consistent sleep and wake schedule
- Morning light exposure
- Evening light reduction
- Caffeine management (cutoff time and reduced total intake)
- Cool, dark, quiet bedroom
Additional priorities based on your specific issues:
If you can’t fall asleep (sleep onset problems):
- Wind-down routine (Foundation 3)
- Stress management (Foundation 10)
- Light exposure timing (Foundation 4)
- Caffeine cutoff even earlier in the day (Foundation 6)
If you can’t stay asleep (sleep maintenance problems):
- Sleep environment optimisation (Foundation 5)
- Eliminate alcohol completely (Foundation 8)
- Further reduce caffeine, possibly eliminate it (Foundation 6)
- Stress management (Foundation 10)
- Body weight assessment if relevant (Foundation 9)
If you’re tired despite seemingly adequate sleep:
- Medical evaluation for sleep disorders
- Body weight assessment (Foundation 9)
- Sleep environment (Foundation 5)
- Schedule consistency (Foundation 2)
- Exercise (Foundation 7)
If you’re highly stressed or anxious:
- Stress management becomes your top priority (Foundation 10)
- Wind-down routine (Foundation 3)
- Exercise (Foundation 7)
- Light exposure (Foundation 4)
Step 2: Choose Your Starting Habits
Don’t try to implement everything at once. Success comes from consistency with a manageable number of changes, not from attempting perfection across all ten foundations. Select 2-5 habits to start:
Always include at least 2-3 from the high-priority universal list. Then add 1-2 specific to your main issue. Track your compliance with these habits and your sleep quality.
Example starting combinations that work well:
Foundation building: Consistent schedule + morning light + caffeine cutoff + cool dark room (4 habits covering the absolute essentials)
Can’t fall asleep: Consistent schedule + wind-down routine + evening dimming + caffeine cutoff + stress management (5 habits targeting sleep onset)
Can’t stay asleep: Consistent schedule + sleep environment optimisation + eliminate alcohol and reduce caffeine + stress management (4 habits targeting sleep maintenance)
Poor sleep despite adequate duration: Morning light + evening dimming + cool dark room + exercise + consistency (5 habits improving sleep quality)
Step 3: Implementation Timeline
Week 1-2: Foundation Building
Implement your chosen 2-5 habits. Track your sleep consistently. Note what time you go to bed, what time you fall asleep (approximately), whether you wake during the night, what time you wake up, and how you feel. Also track compliance with your chosen habits (did you stick to your schedule? did you get morning light? did you avoid caffeine after your cutoff?).
Be consistent even if you don’t see immediate results. Sleep improvements typically take 1-2 weeks to become noticeable and 4-8 weeks to fully stabilise. Don’t add new habits yet—you’re building consistency with your current practices.
Expect some adjustment period, particularly if you’re making significant changes to your schedule or reducing caffeine. You might feel worse temporarily before you feel better. This is normal, and it passes.
Week 3-4: Assessment and Adjustment
Review your tracking data. What patterns do you notice? Are you falling asleep faster? Waking less during the night? Feeling more rested? Which habits are you maintaining consistently? Which ones are you struggling with?
This is the time for fine-tuning. If your consistent bedtime isn’t working because you’re never sleepy at that time, perhaps it’s too early; adjust it slightly later. If morning light at 7am doesn’t align with your schedule, shift it earlier or later, but maintain consistency. If your wind-down routine feels like a chore, try different activities.
Troubleshoot specific issues. If you’re doing everything right but still struggling to fall asleep, you might need to add a wind-down routine or address stress more aggressively. If you’re falling asleep fine, but waking frequently, focus more on environment and eliminate alcohol.
Celebrate small wins. If you’re falling asleep 15 minutes faster than you were three weeks ago, that’s meaningful progress. If you’re waking one fewer times per night, that matters. Acknowledge improvements even if you haven’t achieved perfect sleep yet.
Week 5-8: Addition and Expansion
If you’ve been consistent with your initial habits and you’re ready to add more, introduce 1-2 additional habits. Perhaps you add a structured wind-down routine if you hadn’t before. Perhaps you add regular exercise if that wasn’t in your initial plan. Perhaps you focus more on dietary improvements.
Continue tracking. By this point you should be seeing noticeable improvements in sleep onset time, number of awakenings, or how you feel upon waking and throughout the day. Sleep should feel easier than it did at the start.
Deepen your existing habits. If you’re doing morning light exposure, perhaps you extend it or make it more consistent. If you have a wind-down routine, perhaps you refine which activities work best. If you’ve improved your sleep environment, perhaps you invest in blackout curtains to upgrade from your sleep mask.
Month 3+: Optimisation and Maintenance
Most of your habits should feel relatively automatic by this point. You’re not relying on willpower, you’re following established routines. Sleep has improved substantially from where you started. Now the work is maintaining what’s working, continuing to refine, and addressing any remaining issues.
Some habits will naturally become non-negotiable parts of your routine. Others might require ongoing attention. That’s fine. The goal is sustainable long-term improvement, not perfect adherence to every recommendation forever.
Continue tracking periodically; perhaps a few days each month rather than daily. This keeps you honest and helps you notice if things are slipping. Monthly reviews allow you to assess overall progress and catch problems early.
Adapt to life changes. Your sleep needs and optimal practices may shift over time as your life circumstances change. Stay flexible within the structure you’ve built.
Step 4: Track and Measure
Consistent tracking throughout this process is essential. You’re looking for patterns and correlations: which habits have the biggest impact? which nights do you sleep best? what differentiates good sleep nights from poor ones?
Track at minimum: bedtime, estimated sleep onset time, nighttime awakenings, wake time, and subjective sleep quality rating (1-10). Also, track compliance with your chosen habits each day.
Look for patterns and correlations. Perhaps you notice you always sleep poorly after drinking alcohol, or after late exercise, or when you skip your wind-down routine, or on nights you had caffeine past 2pm. This information tells you which habits are most critical for your individual sleep.
Adjust based on data, not assumptions or feelings. If the data shows your sleep is actually improving even though you don’t feel dramatically different yet, trust the data and maintain consistency. If the data shows a habit isn’t helping despite weeks of implementation, adjust your approach.
Do monthly reviews where you look back at your tracking over the past 4 weeks. What’s improved? What hasn’t? What habits are you maintaining easily? Which ones are you struggling with? What do you want to focus on next month?
Common Obstacles and Solutions
Even with a good plan, you’ll encounter obstacles. Anticipating these and having strategies prepared increases your likelihood of success.
“I Don’t Have Time”
This is almost always about priorities and trade-offs rather than actual time scarcity. You have 24 hours in a day. If you allocate 8 hours to sleep and your sleep hygiene practices, you still have 16 hours for everything else. The question is whether you’re willing to prioritise sleep over other activities.
Look at where your time actually goes. Most people spend hours per day on social media, television, or other entertainment. If you’re scrolling Instagram for 90 minutes before bed, you have time for a wind-down routine, you’re just not using it for that purpose.
Start with time-neutral habits. Consistent sleep schedule doesn’t require additional time; it’s just consistency. Caffeine cutoff doesn’t take time; it’s a boundary. Morning light exposure can be combined with other activities; have your coffee outside, walk to work, park further away and walk.
Better sleep actually gives you more functional hours. When you sleep well, you’re more productive during waking hours. You accomplish more in less time. The time invested in sleep and sleep hygiene pays dividends in increased capacity during the day.
“My Schedule is Irregular (Shift Work, Travel, etc.)”
Some people genuinely face significant obstacles to maintaining consistent sleep schedules, like shift workers, people who travel frequently across time zones, parents of newborns, medical professionals, and emergency responders. These circumstances don’t make good sleep impossible, but they do require a different approach.
Do what you can within your constraints. Even if you can’t maintain perfectly consistent sleep and wake times due to rotating shifts, you can still manage light exposure strategically, maintain a wind-down routine, optimise your sleep environment, and manage caffeine.
Prioritise what you can control. If your sleep schedule must vary, then focus heavily on the habits that don’t depend on schedule consistency, like the sleep environment, light exposure, caffeine management, wind-down routine, and stress management.
Use light exposure strategically. Light is the most powerful circadian signal. If you’re adjusting to a new time zone or a new shift pattern, aggressive light exposure at the right times can speed adaptation. Bright light when you want to be awake, darkness when you want to sleep.
Consider sleep mask and earplugs essential tools. If you need to sleep during daylight hours or in noisy environments, you can’t rely on your environment naturally supporting sleep. Blackout capability via sleep mask and noise control via earplugs or white noise becomes critical.
Accept some limitations. If you’re a permanent night shift worker, your sleep will likely never be quite as good as it would be on a day schedule; you’re working against your biology. But you can still make it significantly better than it would be without proper sleep hygiene. This is about harm reduction and optimisation within constraints, not achieving perfect sleep.
“My Partner Has Different Sleep Needs”
Sharing a bed with someone whose sleep preferences or needs differ from yours is common and challenging. One person is hot whilst the other is cold. One person needs complete silence while the other is fine with noise. One person wants to go to bed at 10pm, while the other prefers midnight. One person is a restless sleeper who wakes the other repeatedly.
Communication and compromise are essential. Have explicit conversations about sleep needs and priorities. Negotiate. Find solutions that work for both people rather than one person always sacrificing their sleep for the other.
Separate sleep spaces aren’t a relationship failure. Some couples sleep better apart, and there’s no shame in having separate bedrooms or even separate beds in the same room. If sleeping together means both people sleep poorly, then separate sleeping arrangements might be the right choice. Quality of relationship and sleep both matter more than adhering to social expectations about couples sharing a bed.
Use separate blankets if cover-stealing is an issue. Get a larger mattress if space is the problem. Use a mattress with good motion isolation if one partner’s movement disturbs the other. Sleep masks and earplugs can help if one partner needs more darkness or quiet than the other prefers.
Coordinate on major environmental factors. Even if you can’t agree on optimal temperature, you can usually find a compromise that’s tolerable for both. Even if bedtimes differ, you can agree that the bedroom should be dark and quiet after the earlier bedtime, with the later person using a reading light in another room during their wind-down time.
Respect each other’s sleep needs. Your partner’s sleep is as important as yours. Neither person’s needs automatically take priority. Work together to find solutions rather than dismissing each other’s concerns or expecting one person to simply adapt to the other’s preferences.
“I Have Young Children”
Parents of young children, particularly infants and toddlers, face genuine and substantial sleep disruption. Newborns need to feed every few hours. Toddlers wake with nightmares or illness. Children climb into your bed at 3am. This isn’t poor sleep hygiene; it’s just the reality of parenting young children.
Have realistic expectations. You’re in survival mode, and that’s okay. Your sleep will be disrupted for a period of years. Accepting this reality reduces the added stress of feeling like you should be sleeping better or something’s wrong with you for being exhausted.
Do what you can within real constraints. You might not be able to maintain a consistent sleep schedule if you’re up multiple times per night with a baby, but you can still optimise your sleep environment, manage caffeine strategically, and get morning light exposure when possible. Every bit helps.
Prioritise the basics. Focus on consistent wake time (even if bedtime varies), getting some morning light (take the baby outside), keeping caffeine earlier in the day, and maintaining a reasonable sleep environment. Don’t try to implement elaborate wind-down routines or achieve perfect sleep hygiene, just do the fundamentals when possible.
Share nighttime duties with your partner if you have one. Take turns with nighttime wake-ups so each person can have some nights of better sleep. Consider one parent handling all nighttime duties for 2-3 nights whilst the other gets to sleep through, then switching.
Sleep when the baby sleeps when possible. Yes, you have other things to do. But chronic severe sleep deprivation has serious health consequences. Sometimes the dishes and other chores can wait.
Know this phase will pass. Infants don’t stay infants forever. Most sleep disruption from children substantially improves by age 2-4. You will sleep properly again. Focus on getting through this phase rather than achieving optimal sleep.
“I’ve Tried Everything and Nothing Works”
Sometimes people implement sleep hygiene recommendations consistently for months and still have terrible sleep. This warrants asking some more questions.
Have you actually tried everything? Be brutally honest. Did you truly maintain schedule consistency every single day for weeks, or did you mostly stick to it with frequent exceptions? Did you actually eliminate caffeine after noon, or did you keep having afternoon tea because you were tired? Did you create a genuine wind-down routine, or did you scroll your phone right up until lights out, while telling yourself you’d tried wind-down routines?
Most people haven’t actually tried everything consistently. They’ve tried many things inconsistently or half-heartedly. If you genuinely have implemented the core foundations consistently for 8+ weeks with zero improvement, then professional help is warranted.
Have you been consistent for long enough? Sleep improvements typically take several weeks to materialise, and full benefits often take 2-3 months. If you implement changes for a week and give up because nothing’s different yet, you haven’t given it a fair trial.
Have you tracked to identify patterns? Without tracking, you’re operating on impression rather than data. Your impression might be that nothing’s working, while the data shows modest but meaningful improvements. Or the tracking might reveal that you’re sleeping poorly, specifically on nights when you violate certain habits, giving you clear information about what matters most for your individual sleep.
Time to see a professional. If you’ve genuinely implemented proper sleep hygiene consistently for 2+ months, tracked your sleep, and seen no improvement whatsoever, then you likely have an underlying issue that requires professional help—possibly a sleep disorder like sleep apnoea, possibly a mental health condition like anxiety or depression, possibly a medical condition affecting sleep.
Don’t give up, but do seek help. Many sleep disorders are highly treatable once properly diagnosed. Cognitive behavioural therapy for insomnia (CBT-I) is extremely effective for chronic insomnia. Medication might be appropriate in some situations. But you can’t diagnose or treat these things yourself—you need a doctor, sleep specialist, or therapist.
“I Feel Worse When I Try to Sleep More”
Some people find that attempts to get more sleep actually make them feel worse rather than better. Several potential causes exist.
You might be oversleeping relative to your individual need. Some people genuinely need less than 8 hours. If you’re spending 9+ hours in bed and feeling worse, try reducing to 7.5 hours and see if you feel better. Quality matters more than quantity.
You might be trying to force sleep when you’re not actually sleepy. If you’re going to bed early because you “should” get 8 hours but you’re not tired, you’ll lie awake, becoming increasingly anxious about not sleeping. This performance anxiety about sleep makes sleep harder. Instead, wait until you’re actually sleepy before going to bed, even if that means less total time in bed initially.
Your sleep quality might be poor even though you’re getting adequate duration. If you’re spending 8 hours in bed but experiencing frequent awakenings, sleep apnoea, or otherwise disrupted sleep architecture, you’re not getting 8 hours of restorative sleep. Focus on quality improvements with stuff like environment optimisation, weight management, and potentially medical evaluation.
Try a consistent wake time without forcing your bedtime. Get up at the same time every day, get morning light immediately, and let sleep pressure build naturally throughout the day. Go to bed when you’re actually sleepy rather than forcing yourself to bed at a prescribed time. For many people, this helps establish a natural sleep drive and reduces sleep-related anxiety.
“I’m Anxious About Not Sleeping”
Anxiety about sleep creates a vicious cycle, as worrying about sleep makes sleep harder, which increases the worry, which makes sleep even harder. This performance anxiety around sleep is common and extremely frustrating.
This anxiety is making things worse. The more you stress about falling asleep, the more activated your nervous system becomes, the more alert you feel, the harder it is to actually sleep. Anxious rumination about sleep actively prevents sleep.
Practice paradoxical intention. Stop trying so hard to sleep. Accept that some nights will be poor, and that’s genuinely okay. One bad night doesn’t ruin you. Humans are remarkably resilient to occasional poor sleep. The anxiety about poor sleep is often more harmful than the poor sleep itself.
Reduce sleep effort. If you’re lying awake trying to force yourself to sleep, get up. Do something calm and boring in dim light until you feel sleepy, then return to bed. Don’t lie in bed awake for hours, as you’re just training your brain to associate bed with wakefulness and anxiety.
Accept that some nights will be poor. Not every night will be perfect. That’s normal. One bad night or even a bad week is recoverable. Stop catastrophizing about the consequences of poor sleep.
Consider CBT-I or therapy. Cognitive behavioural therapy for insomnia specifically addresses the thought patterns and behaviours that perpetuate sleep anxiety. It’s highly effective. If anxiety about sleep is a major problem for you, working with a therapist trained in CBT-I can be transformative.
“I Need Caffeine to Function”
Many people believe they need substantial caffeine intake to function during the day. Often, this belief is perpetuating the problem rather than solving it.
Caffeine is perpetuating your poor sleep. The caffeine you consume to manage daytime fatigue from poor sleep is disrupting your sleep that night, leading to more fatigue the next day, leading to more caffeine. You’re stuck in a cycle.
You’ll feel worse before you feel better. When you reduce caffeine intake, you’ll experience withdrawal symptoms like headaches, fatigue, difficulty concentrating, and irritability. This lasts roughly one to two weeks. It’s genuinely unpleasant, which is why most people give up during this phase and return to high caffeine consumption. But if you push through, your sleep improves, your natural energy levels improve, and you need less caffeine.
Gradual reduction protocol. Don’t go cold turkey. Reduce your total intake by 25-50mg per day each week. If you’re currently having 400mg daily (roughly 3-4 cups of coffee), drop to 350mg for a week, then 300mg, then 250mg, and so on. This minimises withdrawal symptoms whilst still moving toward lower intake.
Replace with other energy strategies. When you feel tired, instead of reaching for caffeine, try going outside for light exposure, doing brief physical movement, drinking cold water, or having a healthy snack. These strategies address low energy without disrupting sleep.
Give it adequate time. Expect 2-4 weeks of adjustment after you’ve reduced your caffeine intake. Your sleep should noticeably improve during this period, and your natural energy levels will start recovering. By 4-6 weeks, most people find that they actually need less caffeine than they did before because they’re sleeping better.
Better sleep reduces your need for caffeine. This is the positive feedback loop working in your favour. Once your sleep improves, you won’t feel as desperate for caffeine during the day. The initial period is difficult, but the long-term outcome is more energy with less dependence on stimulants.
When to Seek Professional Help
Now, while sleep hygiene can solve or substantially improve most sleep problems for most people, but not all sleep issues are pure sleep hygiene problems. Some require medical evaluation and treatment. Knowing when to seek professional help is important.
Signs You Need Medical Evaluation
Loud snoring with gasping or choking: This suggests possible sleep apnoea, where your airway repeatedly becomes blocked during sleep, causing breathing pauses and oxygen desaturation. Sleep apnoea requires medical diagnosis and treatment, typically with CPAP therapy or oral appliances.
Observed breathing pauses during sleep: If your partner or family members have noticed that you stop breathing for periods during sleep, medical evaluation is essential. Untreated sleep apnoea has serious health consequences beyond just poor sleep.
Extreme daytime sleepiness despite adequate time in bed: If you’re spending 8+ hours in bed and still overwhelmingly sleepy during the day (struggling to stay awake at work and/or falling asleep during meetings or while driving), this suggests either very poor sleep quality (possibly due to apnoea) or a sleep disorder like narcolepsy.
Falling asleep uncontrollably during the day: If you fall asleep in situations where most people would have no difficulty staying awake, like during conversations, while eating, or while actively engaged in activities, this warrants evaluation for disorders like narcolepsy.
Restless legs or uncomfortable sensations preventing sleep: Restless legs syndrome causes uncomfortable sensations in the legs (often described as crawling, tingling, or aching) that create an irresistible urge to move them, particularly when lying down. This prevents sleep onset and requires medical treatment.
Acting out dreams or unusual movements during sleep: REM sleep behaviour disorder causes people to physically act out dreams, sometimes violently. Periodic limb movement disorder causes repetitive limb movements during sleep. These require medical evaluation.
No improvement after 8+ weeks of solid sleep hygiene: If you’ve genuinely implemented proper sleep hygiene consistently for 2+ months and seen zero improvement, something else is going on. Chronic insomnia might require CBT-I or medication. Underlying medical conditions might be interfering. Mental health issues might need addressing. Don’t keep struggling alone; get professional help.
Types of Professionals
Primary Care Physician: This is your first stop for most sleep concerns. Your GP can evaluate whether your sleep issues might be related to other health conditions, can screen for sleep disorders, can order sleep studies if warranted, and can refer you to specialists when needed. Many sleep problems can be addressed at the primary care level without needing specialists.
Sleep Medicine Specialist: Physicians who specialise in sleep disorders. They interpret sleep studies, diagnose conditions like sleep apnoea, narcolepsy, and restless legs syndrome, and can provide specialised treatment. You typically need a referral from your primary care physician to see a sleep specialist.
Therapist or Psychologist: If stress, anxiety, depression, or other mental health issues are substantially interfering with your sleep, therapy can be enormously helpful. Cognitive behavioural therapy addresses thought patterns and behaviours that perpetuate sleep problems. Therapists can also provide CBT-I specifically for chronic insomnia.
Sleep Studies: Sleep studies (polysomnography) are specialised tests where you sleep in a lab or at home while wearing sensors that monitor brain activity, breathing, oxygen levels, heart rate, and movement. These are used to diagnose sleep disorders like apnoea, periodic limb movement disorder, or unusual sleep patterns. Your doctor will determine if you need a sleep study based on your symptoms.
Cognitive Behavioural Therapy for Insomnia (CBT-I)
CBT-I is the gold standard treatment for chronic insomnia. It’s as effective as sleep medication for treating insomnia, with much longer-lasting results and no side effects or dependence concerns. CBT-I typically consists of 6-8 sessions with a trained therapist.
The treatment includes several components: sleep restriction therapy (temporarily limiting time in bed to match actual sleep time, then gradually increasing as sleep efficiency improves), stimulus control (strengthening the association between bed and sleep), cognitive therapy (addressing thoughts and beliefs about sleep that increase anxiety), and sleep hygiene education. It’s highly structured and evidence-based.
If you have chronic insomnia that hasn’t responded to sleep hygiene improvements, CBT-I should be your next step before considering long-term medication use. Most people see substantial improvements within a few weeks, and the skills you learn continue working long after treatment ends.
Medications
Sleep medications can be appropriate in some situations, like acute insomnia following a traumatic event, short-term use during a particularly stressful period, or as a bridge while implementing CBT-I. They’re not typically a good long-term solution for chronic sleep problems.
Most sleep medications have significant downsides: they alter sleep architecture (you might be unconscious for 8 hours but not getting natural restorative sleep), they often create dependency and tolerance (requiring higher doses over time), they often have side effects, and they don’t address the underlying causes of poor sleep.
If you’re considering sleep medication, work closely with your prescriber. Combine medication with sleep hygiene improvements rather than relying solely on medication. Have a plan for discontinuation rather than assuming you’ll take medication indefinitely. Consider CBT-I as an alternative or complementary approach.
Various options exist, including prescription medications (benzodiazepines, Z-drugs like zolpidem, sedating antidepressants, orexin antagonists) and over-the-counter options (antihistamines like diphenhydramine, melatonin). Each has different mechanisms, efficacy, and side effect profiles. This is a conversation to have with a qualified healthcare provider, not something to self-medicate.
The Long Game: Maintaining Good Sleep
Sleep improvement isn’t a project with a defined endpoint; it’s an ongoing practice that needs to be maintained long-term. Here’s how to ensure your improvements last.
Building Lasting Habits
Consistency creates automaticity. The sleep hygiene habits that feel difficult and require willpower initially become progressively easier with repetition. After a few months of going to bed at the same time every night, it starts feeling natural rather than forced. After consistently getting morning light, your body starts expecting it, and you feel drawn to go outside. Your wind-down routine becomes a comforting ritual rather than a chore.
Habits become easier over time, not harder. This is the opposite of what most people assume. They think maintaining good sleep hygiene will require constant willpower forever. In reality, like most things health and fitness, the initial weeks are hardest. As habits solidify and the positive feedback loop kicks in, maintaining them becomes progressively easier and easier.
Continue tracking periodically. You don’t necessarily need to track daily forever, but occasional tracking, perhaps a week each month or whenever you feel your sleep slipping, keeps you honest and helps you notice problems before they become entrenched.
Maintain your non-negotiables. Some habits are absolutely essential for your sleep and can’t be compromised without consequences. For most people, schedule consistency and light exposure are non-negotiable. Identify your personal non-negotiables and protect them.
Allow some flexibility in lower priority areas. Not everything needs to be perfect all the time. If your wind-down routine occasionally gets shortened or skipped because of life circumstances, that’s fine. If you occasionally have caffeine slightly past your cutoff time, one instance won’t ruin your sleep. Rigid perfectionism is neither sustainable nor necessary.
Adapting Over Time
Sleep needs and optimal practices change as you age, as your life circumstances change, and as you learn more about what works for your individual biology. Stay flexible.
Life circumstances change. You might have children, change jobs, move to a different climate, develop health conditions, or experience other major life changes that affect sleep. When this happens, revisit your sleep hygiene practices and adjust as needed. The fundamentals remain the same, but the specific implementation might need to shift.
Sleep needs change with age. Older adults often need slightly less sleep and experience changes in sleep architecture. Teenagers need more sleep than adults. Pregnant women need more sleep. What works at age 25 might need adjustment at age 45 or 65.
Return to basics when things slip. Even with well-established habits, life occasionally disrupts your routine (travel, illness, major stress, irregular schedules, etc.). When this happens, and your sleep suffers, return to the absolute basics: consistent wake time, morning light, evening dimming, reasonable bedtime, and a dark, cool room. These core habits can usually get you back on track quickly.
Flexibility within structure. You need structure and consistency for good sleep, but you also need some flexibility for life to be worth living. Find the balance where you maintain enough structure that your sleep stays good, but enough flexibility that you’re not anxiously rigid about every detail.
Dealing with Setbacks
Even with good habits, you’ll occasionally have poor sleep. One bad night is completely normal and fine. Your body is resilient to occasional poor sleep. Don’t catastrophise about a single rough night.
Even a bad week is recoverable. If you have a week of disrupted sleep due to illness, travel, unusual stress, or whatever else, you haven’t ruined your sleep forever. Return to your normal routine, and your sleep will typically re-stabilise within a few days.
Don’t abandon everything because of occasional lapses. This is the all-or-nothing thinking trap. You stay up late one night and think you’ve ruined your sleep schedule, so you abandon your schedule entirely. You skip your morning light exposure for a few days and feel like you’ve failed, so you stop bothering. Don’t do this. One lapse doesn’t mean failure. Just return to your habits the next day.
Learn from disruptions. Sometimes poor sleep gives you useful information. If you consistently sleep poorly after certain foods, late exercise, alcohol, caffeine past a certain time, or stressful events, you’re learning what your individual sleep is most sensitive to. Use this information to refine your practices.
Protecting Your Sleep
Maintaining good sleep long-term requires actively protecting it against pressures and temptations that would undermine it.
Say no to late-night commitments when appropriate. Not everything social needs to be accepted. Not every invitation needs to be honoured. Sometimes protecting your sleep means declining things that would keep you out late or disrupt your schedule.
Communicate your needs. Let people know that sleep is a priority for you. Your friends and family might not naturally consider your sleep schedule when planning things, but if you communicate about it, most people are understanding.
Travel planning. When you travel, particularly across time zones, plan your light exposure strategically to help adaptation. Bring sleep masks and earplugs. Maintain as much schedule consistency as possible given the circumstances.
Holiday survival. Holidays and celebrations often involve staying up late, alcohol, irregular eating, and disrupted routines. You don’t need to be rigidly perfect, but you can make choices that minimise sleep disruption, such as limiting alcohol, getting morning light even when staying somewhere unfamiliar, and returning to your normal schedule as quickly as possible afterwards.
Making sleep a priority isn’t selfish. Your sleep affects your health, mood, relationships, work performance, and overall quality of life. Taking care of your sleep is taking care of yourself, which allows you to be more present and capable in all areas of life. It’s not selfish; it’s responsible.
Continuing Education
Sleep science evolves. New research emerges regularly, and recommendations shift as we learn more. Stay curious but appropriately sceptical.
Revisit the articles in this series periodically. As you gain experience with implementing sleep hygiene, re-reading the detailed articles on specific foundations can give you additional insights you didn’t notice initially.
Join communities. Online or in-person groups focused on sleep health can provide support, accountability, and practical tips from others working on similar issues.
Share your wins and struggles. Talking about sleep with friends and family not only helps you but often helps them recognise their own sleep issues. Sharing strategies that have worked for you might help someone else.
Be appropriately sceptical of new trends. Every few years, a new sleep optimisation trend emerges, whether it’s particular supplements, specific protocols, sleep tracking gadgets, or elaborate routines. Most of these are either marketing hype or marginal optimisations that don’t matter if you haven’t mastered the basics. Focus on the fundamentals.
Foundational Sleep Hygiene Overview
Better sleep isn’t just about feeling less tired, though that certainly matters. It’s about expanding your capacity to live well.
When you sleep properly, everything else in your life becomes easier. You have more energy for exercise. You make better food choices because your appetite regulation and willpower are intact. You manage stress more effectively because your emotional regulation is better. You think more clearly and make better decisions. You’re more patient and present in your relationships. Your immune system functions properly. Your body recovers and repairs effectively.
Good sleep isn’t a luxury that only matters after you’ve sorted everything else out. It’s the foundation that makes sorting everything else out possible. Trying to improve your health, advance your career, build relationships, or pursue meaningful goals while chronically sleep-deprived is like trying to build a house on sand. It’s possible but unnecessarily difficult, and the results are unstable.
Sleep improvement creates positive cascades throughout your life. When you start sleeping better, you naturally have more energy to exercise. Exercise improves your sleep further and also helps with weight management and stress. Better sleep and more exercise improve your appetite regulation, making healthy eating easier. Better diet improves sleep. Better sleep improves stress management capacity, which reduces sleep disruption from stress. Each improvement reinforces the others.
This positive spiral is one of the most powerful forces in the health improvement world, but it requires initial momentum. The start is hardest because you’re working against the negative spiral you’ve been stuck in. But once you break through and establish positive momentum, maintaining it becomes progressively easier. The habits that felt like they required enormous willpower at the beginning become nearly automatic. The sleep quality that felt impossible becomes your new normal.
This isn’t just for high performers trying to optimise every aspect of life. This isn’t just for when you have time after sorting out everything else. This isn’t something to worry about later when you’re less busy. Good sleep matters right now, for you, regardless of your circumstances or goals.
Sleep is a fundamental human need, as essential as food and water. You wouldn’t accept chronic hunger as inevitable or assume you just don’t need food like other people do. Don’t accept chronic poor sleep as inevitable either. You deserve to sleep well. Your body needs it. Your mind needs it. Your life will be measurably better when you sleep properly.
It’s worth the effort. Yes, improving sleep requires making some changes that might feel inconvenient. Yes, it requires prioritising sleep over other things you currently do. Yes, it requires consistency and discipline. But the return on investment is extraordinary. Better sleep improves essentially every domain of your life. Few interventions offer such broad and substantial benefits.
If you’re at the beginning of this journey, implementing sleep hygiene recommendations probably feels daunting. You’re reading about all these habits and wondering how you’ll possibly maintain them. You’re sceptical that they’ll work. You’re worried about the initial discomfort of changing your routine.
And, unfortunately, the start is genuinely the hardest part. The first few weeks require real effort and discipline. You’re establishing new habits while you’re still tired from poor sleep. You’re working against momentum and entrenched patterns. It feels difficult because it is difficult.
But habits become automatic. After a few weeks of consistent practice, going to bed at the same time doesn’t require active decision-making; it’s just what you do. Getting morning light becomes a pleasant ritual rather than a chore. Your wind-down routine becomes something you look forward to rather than something you force yourself through.
Sleep improvements reduce the willpower needed for everything else. Once you’re sleeping properly, maintaining healthy habits requires less effort because you have more mental resources available. The discipline that felt impossible when you were exhausted becomes manageable when you’re well-rested.
The positive feedback loop kicks in. Each small improvement makes the next improvement easier. Sleep better → exercise more easily → sleep better → eat healthier → sleep better → manage stress better → sleep better. The spiral accelerates in a positive direction.
Future you will thank present you. The person you’ll be in three months, six months, a year, living with good sleep, more energy, better health, and expanded capacity, will be deeply grateful that present you was willing to do the difficult work of changing these habits now. By implementing the foundational sleep hygiene habits, you’re not just improving your sleep, you’re investing in your future self’s ability to live well.
As with everything, there is always more to learn, and we haven’t even begun to scratch the surface with all this stuff. However, if you are interested in staying up to date with all our content, we recommend subscribing to our newsletter and bookmarking our free content page. We do have a lot of content on sleep in our sleep hub.
You can read the rest of the articles in this series if you want to go on a deeper dive by clicking the appropriate link:
- What Does Sleep Do?
- Understanding Sleep Architecture: What Actually Happens When You Sleep
- Sleep Regulation: Understanding Your Sleep-Wake Cycle
- How Much Sleep Do You Need?
- Tracking Your Sleep: Foundational Sleep Hygiene
- Consistent Sleep and Wake Times: Foundational Sleep Hygiene
- Wind Down Routine: Foundational Sleep Hygiene
- Light Exposure Management: Foundational Sleep Hygiene
- Sleep Environment Optimisation: Foundational Sleep Hygiene
- Stimulant Management: Foundational Sleep Hygiene
- Exercise and Sleep: Foundational Sleep Hygiene
- Nutrition and Sleep: Foundational Sleep Hygiene
- Body Weight Management: Foundational Sleep Hygiene
- Stress Management and Sleep: Foundational Sleep Hygiene
If you would like more help with your training (or nutrition), we do also have online coaching spaces available.
We also recommend reading our foundational nutrition articles, along with our foundational articles on exercise and stress management, if you really want to learn more about how to optimise your lifestyle. If you want even more free information on sleep, you can follow us on Instagram, YouTube or listen to the podcast, where we discuss all the little intricacies of exercise.
Finally, if you want to learn how to coach nutrition, then consider our Nutrition Coach Certification course. We do also have an exercise program design course, if you are a coach who wants to learn more about effective program design and how to coach it. We do have other courses available too, notably as a sleep course. If you don’t understand something, or you just need clarification, you can always reach out to us on Instagram or via email.
References and Further Reading
Vyazovskiy, V. (2015). Sleep, recovery, and metaregulation: explaining the benefits of sleep. Nature and Science of Sleep, 171. http://doi.org/10.2147/nss.s54036
Sharma, S., & Kavuru, M. (2010). Sleep and Metabolism: An Overview. International Journal of Endocrinology, 2010, 1–12. http://doi.org/10.1155/2010/270832
Yoo, S.-S., Gujar, N., Hu, P., Jolesz, F. A., & Walker, M. P. (2007). The human emotional brain without sleep — a prefrontal amygdala disconnect. Current Biology, 17(20). http://doi.org/10.1016/j.cub.2007.08.007
Copinschi G. Metabolic and endocrine effects of sleep deprivation. Essent Psychopharmacol. 2005;6(6):341-7. PMID: 16459757. https://pubmed.ncbi.nlm.nih.gov/16459757/
Spiegel, K., Leproult, R., L’Hermite-Balériaux, M., Copinschi, G., Penev, P. D., & Cauter, E. V. (2004). Leptin Levels Are Dependent on Sleep Duration: Relationships with Sympathovagal Balance, Carbohydrate Regulation, Cortisol, and Thyrotropin. The Journal of Clinical Endocrinology & Metabolism, 89(11), 5762–5771. http://doi.org/10.1210/jc.2004-1003
Nedeltcheva, A. V., Kilkus, J. M., Imperial, J., Kasza, K., Schoeller, D. A., & Penev, P. D. (2008). Sleep curtailment is accompanied by increased intake of calories from snacks. The American Journal of Clinical Nutrition, 89(1), 126–133. http://doi.org/10.3945/ajcn.2008.26574
Mullington, J. M., Chan, J. L., Dongen, H. P. A. V., Szuba, M. P., Samaras, J., Price, N. J., … Mantzoros, C. S. (2003). Sleep Loss Reduces Diurnal Rhythm Amplitude of Leptin in Healthy Men. Journal of Neuroendocrinology, 15(9), 851–854. http://doi.org/10.1046/j.1365-2826.2003.01069.x
Leproult, R., & Cauter, E. V. (2009). Role of Sleep and Sleep Loss in Hormonal Release and Metabolism. Pediatric Neuroendocrinology Endocrine Development, 11–21. http://doi.org/10.1159/000262524
Spaeth, A. M., Dinges, D. F., & Goel, N. (2013). Effects of Experimental Sleep Restriction on Weight Gain, Caloric Intake, and Meal Timing in Healthy Adults. Sleep, 36(7), 981–990. http://doi.org/10.5665/sleep.2792
Calvin, A. D., Carter, R. E., Adachi, T., Macedo, P. G., Albuquerque, F. N., Walt, C. V. D., … Somers, V. K. (2013). Effects of Experimental Sleep Restriction on Caloric Intake and Activity Energy Expenditure. Chest, 144(1), 79–86. http://doi.org/10.1378/chest.12-2829
Markwald, R. R., Melanson, E. L., Smith, M. R., Higgins, J., Perreault, L., Eckel, R. H., & Wright, K. P. (2013). Impact of insufficient sleep on total daily energy expenditure, food intake, and weight gain. Proceedings of the National Academy of Sciences, 110(14), 5695–5700. http://doi.org/10.1073/pnas.1216951110
Cauter, E. V., Spiegel, K., Tasali, E., & Leproult, R. (2008). Metabolic consequences of sleep and sleep loss. Sleep Medicine, 9. http://doi.org/10.1016/s1389-9457(08)70013-3
Spiegel, K., Leproult, R., & Cauter, E. V. (1999). Impact of sleep debt on metabolic and endocrine function. The Lancet, 354(9188), 1435–1439. http://doi.org/10.1016/s0140-6736(99)01376-8
Ness, K. M., Strayer, S. M., Nahmod, N. G., Schade, M. M., Chang, A.-M., Shearer, G. C., & Buxton, O. M. (2019). Four nights of sleep restriction suppress the postprandial lipemic response and decrease satiety. Journal of Lipid Research, 60(11), 1935–1945. http://doi.org/10.1194/jlr.p094375
Hirotsu, C., Tufik, S., & Andersen, M. L. (2015). Interactions between sleep, stress, and metabolism: From physiological to pathological conditions. Sleep Science, 8(3), 143–152. http://doi.org/10.1016/j.slsci.2015.09.002
Morselli, L., Leproult, R., Balbo, M., & Spiegel, K. (2010). Role of sleep duration in the regulation of glucose metabolism and appetite. Best Practice & Research Clinical Endocrinology & Metabolism, 24(5), 687–702. http://doi.org/10.1016/j.beem.2010.07.005
Lamon, S., Morabito, A., Arentson-Lantz, E., Knowles, O., Vincent, G. E., Condo, D., … Aisbett, B. (2020). The effect of acute sleep deprivation on skeletal muscle protein synthesis and the hormonal environment. http://doi.org/10.1101/2020.03.09.984666
Lipton, J. O., & Sahin, M. (2014). The Neurology of mTOR. Neuron, 84(2), 275–291. http://doi.org/10.1016/j.neuron.2014.09.034
Tudor, J. C., Davis, E. J., Peixoto, L., Wimmer, M. E., Tilborg, E. V., Park, A. J., … Abel, T. (2016). Sleep deprivation impairs memory by attenuating mTORC1-dependent protein synthesis. Science Signaling, 9(425). http://doi.org/10.1126/scisignal.aad4949
Dattilo, M., Antunes, H., Medeiros, A., Neto, M. M., Souza, H., Tufik, S., & Mello, M. D. (2011). Sleep and muscle recovery: Endocrinological and molecular basis for a new and promising hypothesis. Medical Hypotheses, 77(2), 220–222. http://doi.org/10.1016/j.mehy.2011.04.017
Thornton, S. N., & Trabalon, M. (2014). Chronic dehydration is associated with obstructive sleep apnoea syndrome. Clinical Science, 128(3), 225–225. http://doi.org/10.1042/cs20140496
Rosinger, A. Y., Chang, A.-M., Buxton, O. M., Li, J., Wu, S., & Gao, X. (2018). Short sleep duration is associated with inadequate hydration: cross-cultural evidence from US and Chinese adults. Sleep, 42(2). http://doi.org/10.1093/sleep/zsy210
Watson, A. M. (2017). Sleep and Athletic Performance. Current Sports Medicine Reports, 16(6), 413–418. http://doi.org/10.1249/jsr.0000000000000418
Bonnar, D., Bartel, K., Kakoschke, N., & Lang, C. (2018). Sleep Interventions Designed to Improve Athletic Performance and Recovery: A Systematic Review of Current Approaches. Sports Medicine, 48(3), 683–703. http://doi.org/10.1007/s40279-017-0832-x
Saidi, O., Davenne, D., Lehorgne, C., & Duché, P. (2020). Effects of timing of moderate exercise in the evening on sleep and subsequent dietary intake in lean, young, healthy adults: randomized crossover study. European Journal of Applied Physiology, 120(7), 1551–1562. http://doi.org/10.1007/s00421-020-04386-6
Abedelmalek, S., Chtourou, H., Aloui, A., Aouichaoui, C., Souissi, N., & Tabka, Z. (2012). Effect of time of day and partial sleep deprivation on plasma concentrations of IL-6 during a short-term maximal performance. European Journal of Applied Physiology, 113(1), 241–248. http://doi.org/10.1007/s00421-012-2432-7
Azboy, O., & Kaygisiz, Z. (2009). Effects of sleep deprivation on cardiorespiratory functions of the runners and volleyball players during rest and exercise. Acta Physiologica Hungarica, 96(1), 29–36. http://doi.org/10.1556/aphysiol.96.2009.1.3
Bird, S. P. (2013). Sleep, Recovery, and Athletic Performance. Strength and Conditioning Journal, 35(5), 43–47. http://doi.org/10.1519/ssc.0b013e3182a62e2f
Blumert, P. A., Crum, A. J., Ernsting, M., Volek, J. S., Hollander, D. B., Haff, E. E., & Haff, G. G. (2007). The Acute Effects of Twenty-Four Hours of Sleep Loss on the Performance of National-Caliber Male Collegiate Weightlifters. The Journal of Strength and Conditioning Research, 21(4), 1146. http://doi.org/10.1519/r-21606.1
Chase, J. D., Roberson, P. A., Saunders, M. J., Hargens, T. A., Womack, C. J., & Luden, N. D. (2017). One night of sleep restriction following heavy exercise impairs 3-km cycling time-trial performance in the morning. Applied Physiology, Nutrition, and Metabolism, 42(9), 909–915. http://doi.org/10.1139/apnm-2016-0698
Edwards, B. J., & Waterhouse, J. (2009). Effects of One Night of Partial Sleep Deprivation upon Diurnal Rhythms of Accuracy and Consistency in Throwing Darts. Chronobiology International, 26(4), 756–768. http://doi.org/10.1080/07420520902929037
Fullagar, H. H. K., Skorski, S., Duffield, R., Hammes, D., Coutts, A. J., & Meyer, T. (2014). Sleep and Athletic Performance: The Effects of Sleep Loss on Exercise Performance, and Physiological and Cognitive Responses to Exercise. Sports Medicine, 45(2), 161–186. http://doi.org/10.1007/s40279-014-0260-0
Gupta, L., Morgan, K., & Gilchrist, S. (2016). Does Elite Sport Degrade Sleep Quality? A Systematic Review. Sports Medicine, 47(7), 1317–1333. http://doi.org/10.1007/s40279-016-0650-6
Hausswirth, C., Louis, J., Aubry, A., Bonnet, G., Duffield, R., & Meur, Y. L. (2014). Evidence of Disturbed Sleep and Increased Illness in Overreached Endurance Athletes. Medicine & Science in Sports & Exercise, 46(5), 1036–1045. http://doi.org/10.1249/mss.0000000000000177
Mah, C. D., Mah, K. E., Kezirian, E. J., & Dement, W. C. (2011). The Effects of Sleep Extension on the Athletic Performance of Collegiate Basketball Players. Sleep, 34(7), 943–950. http://doi.org/10.5665/sleep.1132
Milewski, M. D., Skaggs, D. L., Bishop, G. A., Pace, J. L., Ibrahim, D. A., Wren, T. A., & Barzdukas, A. (2014). Chronic Lack of Sleep is Associated With Increased Sports Injuries in Adolescent Athletes. Journal of Pediatric Orthopaedics, 34(2), 129–133. http://doi.org/10.1097/bpo.0000000000000151
Mougin, F., Bourdin, H., Simon-Rigaud, M., Didier, J., Toubin, G., & Kantelip, J. (1996). Effects of a Selective Sleep Deprivation on Subsequent Anaerobic Performance. International Journal of Sports Medicine, 17(02), 115–119. http://doi.org/10.1055/s-2007-972818
Oliver, S. J., Costa, R. J. S., Laing, S. J., Bilzon, J. L. J., & Walsh, N. P. (2009). One night of sleep deprivation decreases treadmill endurance performance. European Journal of Applied Physiology, 107(2), 155–161. http://doi.org/10.1007/s00421-009-1103-9
Pallesen, S., Gundersen, H. S., Kristoffersen, M., Bjorvatn, B., Thun, E., & Harris, A. (2017). The Effects of Sleep Deprivation on Soccer Skills. Perceptual and Motor Skills, 124(4), 812–829. http://doi.org/10.1177/0031512517707412
Reilly, T., & Piercy, M. (1994). The effect of partial sleep deprivation on weight-lifting performance. Ergonomics, 37(1), 107–115. http://doi.org/10.1080/00140139408963628
Rossa, K. R., Smith, S. S., Allan, A. C., & Sullivan, K. A. (2014). The Effects of Sleep Restriction on Executive Inhibitory Control and Affect in Young Adults. Journal of Adolescent Health, 55(2), 287–292. http://doi.org/10.1016/j.jadohealth.2013.12.034
Sargent, C., & Roach, G. D. (2016). Sleep duration is reduced in elite athletes following night-time competition. Chronobiology International, 33(6), 667–670. http://doi.org/10.3109/07420528.2016.1167715
Skein, M., Duffield, R., Edge, J., Short, M. J., & Mündel, T. (2011). Intermittent-Sprint Performance and Muscle Glycogen after 30 h of Sleep Deprivation. Medicine & Science in Sports & Exercise, 43(7), 1301–1311. http://doi.org/10.1249/mss.0b013e31820abc5a
Souissi, N., Sesboüé, B., Gauthier, A., Larue, J., & Davenne, D. (2003). Effects of one nights sleep deprivation on anaerobic performance the following day. European Journal of Applied Physiology, 89(3), 359–366. http://doi.org/10.1007/s00421-003-0793-7
Caia, J., Kelly, V. G., & Halson, S. L. (2017). The role of sleep in maximising performance in elite athletes. Sport, Recovery, and Performance, 151–167. http://doi.org/10.4324/9781315268149-11
Alley, J. R., Mazzochi, J. W., Smith, C. J., Morris, D. M., & Collier, S. R. (2015). Effects of Resistance Exercise Timing on Sleep Architecture and Nocturnal Blood Pressure. Journal of Strength and Conditioning Research, 29(5), 1378–1385. http://doi.org/10.1519/jsc.0000000000000750
Kovacevic, A., Mavros, Y., Heisz, J. J., & Singh, M. A. F. (2018). The effect of resistance exercise on sleep: A systematic review of randomized controlled trials. Sleep Medicine Reviews, 39, 52–68. http://doi.org/10.1016/j.smrv.2017.07.002
Herrick, J. E., Puri, S., & Richards, K. C. (2017). Resistance training does not alter same-day sleep architecture in institutionalized older adults. Journal of Sleep Research, 27(4). http://doi.org/10.1111/jsr.12590
Edinger, J. D., Morey, M. C., Sullivan, R. J., Higginbotham, M. B., Marsh, G. R., Dailey, D. S., & McCall, W. V. (1993). Aerobic fitness, acute exercise and sleep in older men. Sleep, 16(4), 351-359. https://doi.org/10.1093/sleep/16.4.351
King, A. C. (1997). Moderate-intensity exercise and self-rated quality of sleep in older adults. A randomized controlled trial. JAMA: The Journal of the American Medical Association, 277(1), 32–37. http://doi.org/10.1001/jama.277.1.32
Passos, G. S., Poyares, D., Santana, M. G., Garbuio, S. A., Tufik, S., & Mello, M. T. (2010). Effect of Acute Physical Exercise on Patients with Chronic Primary Insomnia. Journal of Clinical Sleep Medicine, 06(03), 270–275. http://doi.org/10.5664/jcsm.27825
Reid, K. J., Baron, K. G., Lu, B., Naylor, E., Wolfe, L., & Zee, P. C. (2010). Aerobic exercise improves self-reported sleep and quality of life in older adults with insomnia. Sleep Medicine, 11(9), 934–940. http://doi.org/10.1016/j.sleep.2010.04.014
Viana, V. A. R., Esteves, A. M., Boscolo, R. A., Grassmann, V., Santana, M. G., Tufik, S., & Mello, M. T. D. (2011). The effects of a session of resistance training on sleep patterns in the elderly. European Journal of Applied Physiology, 112(7), 2403–2408. http://doi.org/10.1007/s00421-011-2219-2
Herring, M., Kline, C., & Oconnor, P. (2015). Effects of Exercise Training On Self-reported Sleep Among Young Women with Generalized Anxiety Disorder (GAD). European Psychiatry, 30, 465. http://doi.org/10.1016/s0924-9338(15)31893-9
Kredlow, M. A., Capozzoli, M. C., Hearon, B. A., Calkins, A. W., & Otto, M. W. (2015). The effects of physical activity on sleep: a meta-analytic review. Journal of Behavioral Medicine, 38(3), 427–449. http://doi.org/10.1007/s10865-015-9617-6
Yang, P.-Y., Ho, K.-H., Chen, H.-C., & Chien, M.-Y. (2012). Exercise training improves sleep quality in middle-aged and older adults with sleep problems: a systematic review. Journal of Physiotherapy, 58(3), 157–163. http://doi.org/10.1016/s1836-9553(12)70106-6
Kline, C. E., Sui, X., Hall, M. H., Youngstedt, S. D., Blair, S. N., Earnest, C. P., & Church, T. S. (2012). Dose–response effects of exercise training on the subjective sleep quality of postmenopausal women: exploratory analyses of a randomised controlled trial. BMJ Open, 2(4). http://doi.org/10.1136/bmjopen-2012-001044
Fairbrother, K., Cartner, B. W., Triplett, N., Morris, D. M., & Collier, S. R. (2011). The Effects of Aerobic Exercise Timing on Sleep Architecture. Medicine & Science in Sports & Exercise, 43(Suppl 1), 879. http://doi.org/10.1249/01.mss.0000402452.16375.20
Youngstedt, S. D., & Kline, C. E. (2006). Epidemiology of exercise and sleep. Sleep and Biological Rhythms, 4(3), 215–221. http://doi.org/10.1111/j.1479-8425.2006.00235.x
Stenholm, S., Head, J., Kivimäki, M., Hanson, L. L. M., Pentti, J., Rod, N. H., … Vahtera, J. (2018). Sleep Duration and Sleep Disturbances as Predictors of Healthy and Chronic Disease–Free Life Expectancy Between Ages 50 and 75: A Pooled Analysis of Three Cohorts. The Journals of Gerontology: Series A, 74(2), 204–210. http://doi.org/10.1093/gerona/gly01
Xiao, Q., Keadle, S. K., Hollenbeck, A. R., & Matthews, C. E. (2014). Sleep Duration and Total and Cause-Specific Mortality in a Large US Cohort: Interrelationships With Physical Activity, Sedentary Behavior, and Body Mass Index. American Journal of Epidemiology, 180(10), 997–1006. http://doi.org/10.1093/aje/kwu222
Reynolds, A. C., Dorrian, J., Liu, P. Y., Dongen, H. P. A. V., Wittert, G. A., Harmer, L. J., & Banks, S. (2012). Impact of Five Nights of Sleep Restriction on Glucose Metabolism, Leptin and Testosterone in Young Adult Men. PLoS ONE, 7(7). http://doi.org/10.1371/journal.pone.0041218
Åkerstedt, T., Palmblad, J., Torre, B. D. L., Marana, R., & Gillberg, M. (1980). Adrenocortical and Gonadal Steroids During Sleep Deprivation. Sleep, 3(1), 23–30. http://doi.org/10.1093/sleep/3.1.23
Cortés-Gallegos, V., Castañeda, G., Alonso, R., Sojo, I., Carranco, A., Cervantes, C., & Parra, A. (1983). Sleep Deprivation Reduces Circulating Androgens in Healthy Men. Archives of Andrology, 10(1), 33–37. http://doi.org/10.3109/01485018308990167
González-Santos, M. R., Gajá-Rodíguez, O. V., Alonso-Uriarte, R., Sojo-Aranda, I., & Cortés-Gallegos, V. (1989). Sleep Deprivation and Adaptive Hormonal Responses of Healthy Men. Archives of Andrology, 22(3), 203–207. http://doi.org/10.3109/01485018908986773
Penev, P. D. (2007). Association Between Sleep and Morning Testosterone Levels In Older Men. Sleep, 30(4), 427–432. http://doi.org/10.1093/sleep/30.4.427
Kloss, J. D., Perlis, M. L., Zamzow, J. A., Culnan, E. J., & Gracia, C. R. (2015). Sleep, sleep disturbance, and fertility in women. Sleep Medicine Reviews, 22, 78–87. http://doi.org/10.1016/j.smrv.2014.10.005
Mahoney, M. M. (2010). Shift Work, Jet Lag, and Female Reproduction. International Journal of Endocrinology, 2010, 1–9. http://doi.org/10.1155/2010/813764
Labyak, S., Lava, S., Turek, F., & Zee, P. (2002). Effects Of Shiftwork On Sleep And Menstrual Function In Nurses. Health Care for Women International, 23(6-7), 703–714. http://doi.org/10.1080/07399330290107449
Pal, L., Bevilacqua, K., Zeitlian, G., Shu, J., & Santoro, N. (2008). Implications of diminished ovarian reserve (DOR) extend well beyond reproductive concerns. Menopause, 15(6), 1086–1094. http://doi.org/10.1097/gme.0b013e3181728467
Axelsson, G., Rylander, R., & Molin, I. (1989). Outcome of pregnancy in relation to irregular and inconvenient work schedules. Occupational and Environmental Medicine, 46(6), 393–398. http://doi.org/10.1136/oem.46.6.393
Bisanti, L., Olsen, J., Basso, O., Thonneau, P., & Karmaus, W. (1996). Shift Work and Subfecundity: A European Multicenter Study. Journal of Occupational & Environmental Medicine, 38(4), 352–358. http://doi.org/10.1097/00043764-199604000-00012
Rossmanith, W. G. (1998). The impact of sleep on gonadotropin secretion. Gynecological Endocrinology, 12(6), 381–389. http://doi.org/10.3109/09513599809012840
Fernando, S., & Rombauts, L. (2014). Melatonin: shedding light on infertility? – a review of the recent literature. Journal of Ovarian Research, 7(1). http://doi.org/10.1186/s13048-014-0098-y
Rocha, C., Rato, L., Martins, A., Alves, M., & Oliveira, P. (2015). Melatonin and Male Reproductive Health: Relevance of Darkness and Antioxidant Properties. Current Molecular Medicine, 15(4), 299–311. http://doi.org/10.2174/1566524015666150505155530
Song, C., Peng, W., Yin, S., Zhao, J., Fu, B., Zhang, J., … Zhang, Y. (2016). Melatonin improves age-induced fertility decline and attenuates ovarian mitochondrial oxidative stress in mice. Scientific Reports, 6(1). http://doi.org/10.1038/srep35165
Espino, J., Macedo, M., Lozano, G., Ortiz, Á., Rodríguez, C., Rodríguez, A. B., & Bejarano, I. (2019). Impact of Melatonin Supplementation in Women with Unexplained Infertility Undergoing Fertility Treatment. Antioxidants, 8(9), 338. http://doi.org/10.3390/antiox8090338
Tamura, H., Takasaki, A., Taketani, T., Tanabe, M., Kizuka, F., Lee, L., … Sugino, N. (2012). The role of melatonin as an antioxidant in the follicle. Journal of Ovarian Research, 5(1), 5. http://doi.org/10.1186/1757-2215-5-5
Saaresranta, T., & Polo, O. (2003). Sleep-disordered breathing and hormones. European Respiratory Journal, 22(1), 161–172. http://doi.org/10.1183/09031936.03.00062403
Cappuccio, F. P., Cooper, D., Delia, L., Strazzullo, P., & Miller, M. A. (2011). Sleep duration predicts cardiovascular outcomes: a systematic review and meta-analysis of prospective studies. European Heart Journal, 32(12), 1484–1492. http://doi.org/10.1093/eurheartj/ehr007
Jansen, E. C., Dunietz, G. L., Tsimpanouli, M.-E., Guyer, H. M., Shannon, C., Hershner, S. D., … Baylin, A. (2018). Sleep, Diet, and Cardiometabolic Health Investigations: a Systematic Review of Analytic Strategies. Current Nutrition Reports, 7(4), 235–258. http://doi.org/10.1007/s13668-018-0240-3
Knutson, K. L., Cauter, E. V., Rathouz, P. J., Yan, L. L., Hulley, S. B., Liu, K., & Lauderdale, D. S. (2009). Association Between Sleep and Blood Pressure in Midlife. Archives of Internal Medicine, 169(11), 1055. http://doi.org/10.1001/archinternmed.2009.119
Besedovsky, L., Lange, T., & Born, J. (2011). Sleep and immune function. Pflügers Archiv – European Journal of Physiology, 463(1), 121–137. http://doi.org/10.1007/s00424-011-1044-0
Besedovsky, L., Lange, T., & Haack, M. (2019). The Sleep-Immune Crosstalk in Health and Disease. Physiological Reviews, 99(3), 1325–1380. http://doi.org/10.1152/physrev.00010.2018
Orr, W. C., Fass, R., Sundaram, S. S., & Scheimann, A. O. (2020). The effect of sleep on gastrointestinal functioning in common digestive diseases. The Lancet Gastroenterology & Hepatology, 5(6), 616–624. http://doi.org/10.1016/s2468-1253(19)30412-1
Tang, Y., Preuss, F., Turek, F. W., Jakate, S., & Keshavarzian, A. (2009). Sleep deprivation worsens inflammation and delays recovery in a mouse model of colitis. Sleep Medicine, 10(6), 597–603. http://doi.org/10.1016/j.sleep.2008.12.009
Chen, Y., Tan, F., Wei, L., Li, X., Lyu, Z., Feng, X., … Li, N. (2018). Sleep duration and the risk of cancer: a systematic review and meta-analysis including dose–response relationship. BMC Cancer, 18(1). http://doi.org/10.1186/s12885-018-5025-y
Almendros, I., Martinez-Garcia, M. A., Farré, R., & Gozal, D. (2020). Obesity, sleep apnea, and cancer. International Journal of Obesity, 44(8), 1653–1667. http://doi.org/10.1038/s41366-020-0549-z
Erren, T. C., Falaturi, P., Morfeld, P., Knauth, P., Reiter, R. J., & Piekarski, C. (2010). Shift Work and Cancer. Deutsches Aerzteblatt Online. http://doi.org/10.3238/arztebl.2010.0657
Bernert, R. A., Kim, J. S., Iwata, N. G., & Perlis, M. L. (2015). Sleep Disturbances as an Evidence-Based Suicide Risk Factor. Current Psychiatry Reports, 17(3). http://doi.org/10.1007/s11920-015-0554-4
Kim, J.-H., Park, E.-C., Cho, W.-H., Park, J.-Y., Choi, W.-J., & Chang, H.-S. (2013). Association between Total Sleep Duration and Suicidal Ideation among the Korean General Adult Population. Sleep, 36(10), 1563–1572. http://doi.org/10.5665/sleep.3058
Mccall, W. V., & Black, C. G. (2013). The Link Between Suicide and Insomnia: Theoretical Mechanisms. Current Psychiatry Reports, 15(9). http://doi.org/10.1007/s11920-013-0389-9
Li, S. X., Lam, S. P., Zhang, J., Yu, M. W. M., Chan, J. W. Y., Chan, C. S. Y., … Wing, Y.-K. (2016). Sleep Disturbances and Suicide Risk in an 8-Year Longitudinal Study of Schizophrenia-Spectrum Disorders. Sleep, 39(6), 1275–1282. http://doi.org/10.5665/sleep.5852
Littlewood, D. L., Gooding, P., Kyle, S. D., Pratt, D., & Peters, S. (2016). Understanding the role of sleep in suicide risk: qualitative interview study. BMJ Open, 6(8). http://doi.org/10.1136/bmjopen-2016-012113
Lin, H.-T., Lai, C.-H., Perng, H.-J., Chung, C.-H., Wang, C.-C., Chen, W.-L., & Chien, W.-C. (2018). Insomnia as an independent predictor of suicide attempts: a nationwide population-based retrospective cohort study. BMC Psychiatry, 18(1). http://doi.org/10.1186/s12888-018-1702-2
Freeman, D., Sheaves, B., Waite, F., Harvey, A. G., & Harrison, P. J. (2020). Sleep disturbance and psychiatric disorders. The Lancet Psychiatry, 7(7), 628–637. http://doi.org/10.1016/s2215-0366(20)30136-x
Benca, R. M. (1992). Sleep and Psychiatric Disorders. Archives of General Psychiatry, 49(8), 651. http://doi.org/10.1001/archpsyc.1992.01820080059010
Breslau, N., Roth, T., Rosenthal, L., & Andreski, P. (1996). Sleep disturbance and psychiatric disorders: A longitudinal epidemiological study of young Adults. Biological Psychiatry, 39(6), 411–418. http://doi.org/10.1016/0006-3223(95)00188-3
Baglioni, C., Nanovska, S., Regen, W., Spiegelhalder, K., Feige, B., Nissen, C., … Riemann, D. (2016). Sleep and mental disorders: A meta-analysis of polysomnographic research. Psychological Bulletin, 142(9), 969–990. http://doi.org/10.1037/bul0000053
Goldstein, A. N., & Walker, M. P. (2014). The Role of Sleep in Emotional Brain Function. Annual Review of Clinical Psychology, 10(1), 679–708. http://doi.org/10.1146/annurev-clinpsy-032813-153716
Postuma, R. B., Iranzo, A., Hu, M., Högl, B., Boeve, B. F., Manni, R., … Pelletier, A. (2019). Risk and predictors of dementia and parkinsonism in idiopathic REM sleep behaviour disorder: a multicentre study. Brain, 142(3), 744–759. http://doi.org/10.1093/brain/awz030
Wintler, T., Schoch, H., Frank, M. G., & Peixoto, L. (2020). Sleep, brain development, and autism spectrum disorders: Insights from animal models. Journal of Neuroscience Research, 98(6), 1137–1149. http://doi.org/10.1002/jnr.24619
Shokri-Kojori, E., Wang, G.-J., Wiers, C. E., Demiral, S. B., Guo, M., Kim, S. W., … Volkow, N. D. (2018). β-Amyloid accumulation in the human brain after one night of sleep deprivation. Proceedings of the National Academy of Sciences, 115(17), 4483–4488. http://doi.org/10.1073/pnas.1721694115
Mantovani, S., Smith, S. S., Gordon, R., & Osullivan, J. D. (2018). An overview of sleep and circadian dysfunction in Parkinsons disease. Journal of Sleep Research, 27(3). http://doi.org/10.1111/jsr.12673
Malhotra, R. K. (2018). Neurodegenerative Disorders and Sleep. Sleep Medicine Clinics, 13(1), 63–70. http://doi.org/10.1016/j.jsmc.2017.09.006
Huang, L.-B., Tsai, M.-C., Chen, C.-Y., & Hsu, S.-C. (2013). The Effectiveness of Light/Dark Exposure to Treat Insomnia in Female Nurses Undertaking Shift Work during the Evening/Night Shift. Journal of Clinical Sleep Medicine, 09(07), 641–646. http://doi.org/10.5664/jcsm.2824
Zhang, Y., & Papantoniou, K. (2019). Night shift work and its carcinogenicity. The Lancet Oncology, 20(10). http://doi.org/10.1016/s1470-2045(19)30578-9
Perry-Jenkins, M., Goldberg, A. E., Pierce, C. P., & Sayer, A. G. (2007). Shift Work, Role Overload, and the Transition to Parenthood. Journal of Marriage and Family, 69(1), 123–138. http://doi.org/10.1111/j.1741-3737.2006.00349.x
Rodziewicz TL, Hipskind JE. Medical Error Prevention. 2020 May 5. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan–. PMID: 29763131. https://pubmed.ncbi.nlm.nih.gov/29763131/
Tanaka, K., Takahashi, M., Hiro, H., Kakinuma, M., Tanaka, M., Kamata, N., & Miyaoka, H. (2010). Differences in Medical Error Risk among Nurses Working Two- and Three-shift Systems at Teaching Hospitals: A Six-month Prospective Study. Industrial Health, 48(3), 357–364. http://doi.org/10.2486/indhealth.48.357
Admi H, Tzischinsky O, Epstein R, Herer P, Lavie P. Shift work in nursing: is it really a risk factor for nurses’ health and patients’ safety?. Nurs Econ. 2008;26(4):250-257. https://pubmed.ncbi.nlm.nih.gov/18777974/
Clendon, J., & Gibbons, V. (2015). 12h shifts and rates of error among nurses: A systematic review. International Journal of Nursing Studies, 52(7), 1231–1242. http://doi.org/10.1016/j.ijnurstu.2015.03.011
Hammadah, M., Kindya, B. R., Allard‐Ratick, M. P., Jazbeh, S., Eapen, D., Tang, W. W., & Sperling, L. (2017). Navigating air travel and cardiovascular concerns: Is the sky the limit?, Clinical Cardiology, 40 (9), 660–666. http://doi.org/10.1002/clc.22741
Lieber, B. A., Han, J., Appelboom, G., Taylor, B. E., Han, B., Agarwal, N., & Connolly, E. S. (2016). Association of Steroid Use with Deep Venous Thrombosis and Pulmonary Embolism in Neurosurgical Patients: A National Database Analysis. World Neurosurgery, 89, 126–132. http://doi.org/10.1016/j.wneu.2016.01.033
El-Menyar, A., Asim, M., & Al-Thani, H. (2017). Obesity Paradox in Patients With Deep Venous Thrombosis. Clinical and Applied Thrombosis/Hemostasis, 24(6), 986–992. http://doi.org/10.1177/1076029617727858
Klovaite, J., Benn, M., & Nordestgaard, B. G. (2014). Obesity as a causal risk factor for deep venous thrombosis: a Mendelian randomization study. Journal of Internal Medicine, 277(5), 573–584. http://doi.org/10.1111/joim.12299
Davies, H. O., Popplewell, M., Singhal, R., Smith, N., & Bradbury, A. W. (2016). Obesity and lower limb venous disease – The epidemic of phlebesity. Phlebology: The Journal of Venous Disease, 32(4), 227–233. http://doi.org/10.1177/0268355516649333
Liljeqvist, S., Helldén, A., Bergman, U., & Söderberg, M. (2008). Pulmonary embolism associated with the use of anabolic steroids. European Journal of Internal Medicine, 19(3), 214–215. http://doi.org/10.1016/j.ejim.2007.03.016
Linton MF, Yancey PG, Davies SS, Jerome WG (Jay), Linton EF, Vickers KC. The Role of Lipids and Lipoproteins in Atherosclerosis. In: De Groot LJ, Chrousos G, Dungan K, et al., eds. Endotext. South Dartmouth (MA): MDText.com, Inc.; 2000. http://www.ncbi.nlm.nih.gov/books/NBK343489/.
Rescheduling of meals may ease the effects of jet lag. (2017). Nursing Standard, 31(48), 16–16. http://doi.org/10.7748/ns.31.48.16.s17
Ruscitto, C., & Ogden, J. (2016). The impact of an implementation intention to improve mealtimes and reduce jet lag in long-haul cabin crew. Psychology & Health, 32(1), 61–77. http://doi.org/10.1080/08870446.2016.1240174
Reid, K. J., & Abbott, S. M. (2015). Jet Lag and Shift Work Disorder. Sleep Medicine Clinics, 10(4), 523–535. http://doi.org/10.1016/j.jsmc.2015.08.006
Srinivasan, V., Spence, D. W., Pandi-Perumal, S. R., Trakht, I., & Cardinali, D. P. (2008). Jet lag: Therapeutic use of melatonin and possible application of melatonin analogs. Travel Medicine and Infectious Disease, 6(1-2), 17–28. http://doi.org/10.1016/j.tmaid.2007.12.002
Edwards, B. J., Atkinson, G., Waterhouse, J., Reilly, T., Godfrey, R., & Budgett, R. (2000). Use of melatonin in recovery from jet-lag following an eastward flight across 10 time-zones. Ergonomics, 43(10), 1501–1513. http://doi.org/10.1080/001401300750003934
Zee, P. C., & Goldstein, C. A. (2010). Treatment of Shift Work Disorder and Jet Lag. Current Treatment Options in Neurology, 12(5), 396–411. http://doi.org/10.1007/s11940-010-0090-9
https://www.nhlbi.nih.gov/health-topics/circadian-rhythm-disorders
Borodkin, K., & Dagan, Y. (2013). Diagnostic Algorithm for Circadian Rhythm Sleep Disorders. Encyclopedia of Sleep, 66–73. http://doi.org/10.1016/b978-0-12-378610-4.00284-9
Lockley, S. (2013). Special Considerations and Future Directions in Circadian Rhythm Sleep Disorders Diagnosis. Encyclopedia of Sleep, 138–149. http://doi.org/10.1016/b978-0-12-378610-4.00299-0
Crowley, S., & Youngstedt, S. (2013). Pathophysiology, Associations, and Consequences of Circadian Rhythm Sleep Disorder. Encyclopedia of Sleep, 16–21. http://doi.org/10.1016/b978-0-12-378610-4.00266-7
Franken, P., & Dijk, D.-J. (2009). Circadian clock genes and sleep homeostasis. European Journal of Neuroscience, 29(9), 1820–1829. http://doi.org/10.1111/j.1460-9568.2009.06723.x
Burgess, H. J., & Emens, J. S. (2016). Circadian-Based Therapies for Circadian Rhythm Sleep-Wake Disorders. Current Sleep Medicine Reports, 2(3), 158–165. http://doi.org/10.1007/s40675-016-0052-1
Jones, C. R., Huang, A. L., Ptáček, L. J., & Fu, Y.-H. (2013). Genetic basis of human circadian rhythm disorders. Experimental Neurology, 243, 28–33. http://doi.org/10.1016/j.expneurol.2012.07.012
Toh KL. Basic science review on circadian rhythm biology and circadian sleep disorders. Ann Acad Med Singap. 2008;37(8):662-668. https://pubmed.ncbi.nlm.nih.gov/18797559/
Farhud D, Aryan Z. Circadian Rhythm, Lifestyle and Health: A Narrative Review. Iran J Public Health. 2018;47(8):1068-1076. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6123576/
Dodson, E. R., & Zee, P. C. (2010). Therapeutics for Circadian Rhythm Sleep Disorders. Sleep Medicine Clinics, 5(4), 701–715. http://doi.org/10.1016/j.jsmc.2010.08.001
Zhu, L., & Zee, P. C. (2012). Circadian Rhythm Sleep Disorders. Neurologic Clinics, 30(4), 1167–1191. http://doi.org/10.1016/j.ncl.2012.08.011
Kim MJ, Lee JH, Duffy JF. Circadian Rhythm Sleep Disorders. J Clin Outcomes Manag. 2013;20(11):513-528. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4212693/
Zhong, G., Naismith, S. L., Rogers, N. L., & Lewis, S. J. G. (2011). Sleep-wake disturbances in common neurodegenerative diseases: A closer look at selected aspects of the neural circuitry. Journal of the Neurological Sciences, 307(1-2), 9–14. http://doi.org/10.1016/j.jns.2011.04.020
Dijk, D.-J., Boulos, Z., Eastman, C. I., Lewy, A. J., Campbell, S. S., & Terman, M. (1995). Light Treatment for Sleep Disorders: Consensus Report. Journal of Biological Rhythms, 10(2), 113–125. http://doi.org/10.1177/074873049501000204
Barion, A., & Zee, P. C. (2007). A clinical approach to circadian rhythm sleep disorders. Sleep Medicine, 8(6), 566–577. http://doi.org/10.1016/j.sleep.2006.11.017
Horne JA, Ostberg O. A self-assessment questionnaire to determine morningness-eveningness in human circadian rhythms. Int J Chronobiol. 1976;4(2):97-110. https://pubmed.ncbi.nlm.nih.gov/1027738/
Adan, A., & Almirall, H. (1991). Horne & Östberg morningness-eveningness questionnaire: A reduced scale. Personality and Individual Differences, 12(3), 241–253. http://doi.org/10.1016/0191-8869(91)90110-w
Urbán, R., Magyaródi, T., & Rigó, A. (2011). Morningness-Eveningness, Chronotypes and Health-Impairing Behaviors in Adolescents. Chronobiology International, 28(3), 238–247. http://doi.org/10.3109/07420528.2010.549599
https://www.thewep.org/documentations/mctq
Buysse, D. J., Reynolds, C. F., Monk, T. H., Berman, S. R., & Kupfer, D. J. (1989). The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Research, 28(2), 193–213. http://doi.org/10.1016/0165-1781(89)90047-4
Bastien, C. (2001). Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Medicine, 2(4), 297–307. http://doi.org/10.1016/s1389-9457(00)00065-4
Yang, M., Morin, C. M., Schaefer, K., & Wallenstein, G. V. (2009). Interpreting score differences in the Insomnia Severity Index: using health-related outcomes to define the minimally important difference. Current Medical Research and Opinion, 25(10), 2487–2494. http://doi.org/10.1185/03007990903167415
Morin, C. M., Belleville, G., Bélanger, L., & Ivers, H. (2011). The Insomnia Severity Index: Psychometric Indicators to Detect Insomnia Cases and Evaluate Treatment Response. Sleep, 34(5), 601–608. http://doi.org/10.1093/sleep/34.5.601
Castriotta RJ, Wilde MC, Lai JM, Atanasov S, Masel BE, Kuna ST. Prevalence and consequences of sleep disorders in traumatic brain injury. J Clin Sleep Med. 2007;3(4):349-356. https://pubmed.ncbi.nlm.nih.gov/17694722/
Chokroverty S. Overview of sleep & sleep disorders. Indian J Med Res. 2010;131:126-140. https://pubmed.ncbi.nlm.nih.gov/20308738/
Pavlova, M. K., & Latreille, V. (2019). Sleep Disorders. The American Journal of Medicine, 132(3), 292–299. http://doi.org/10.1016/j.amjmed.2018.09.021
Olejniczak, P. W., & Fisch, B. J. (2003). Sleep disorders. Medical Clinics of North America, 87(4), 803–833. http://doi.org/10.1016/s0025-7125(03)00006-3
https://www.nhlbi.nih.gov/health-topics/sleep-apnea
https://clevemed.com/what-is-sleep-apnea/patient-sleep-apnea-screener/
Spicuzza, L., Caruso, D., & Maria, G. D. (2015). Obstructive sleep apnoea syndrome and its management. Therapeutic Advances in Chronic Disease, 6(5), 273–285. http://doi.org/10.1177/2040622315590318
Bixler, E. O., Vgontzas, A. N., Lin, H.-M., Liao, D., Calhoun, S., Fedok, F., … Graff, G. (2008). Blood Pressure Associated With Sleep-Disordered Breathing in a Population Sample of Children. Hypertension, 52(5), 841–846. http://doi.org/10.1161/hypertensionaha.108.116756
Campos, A. I., García-Marín, L. M., Byrne, E. M., Martin, N. G., Cuéllar-Partida, G., & Rentería, M. E. (2020). Insights into the aetiology of snoring from observational and genetic investigations in the UK Biobank. Nature Communications, 11(1). http://doi.org/10.1038/s41467-020-14625-1
Morgenthaler, T. I., Kagramanov, V., Hanak, V., & Decker, P. A. (2006). Complex Sleep Apnea Syndrome: Is It a Unique Clinical Syndrome? Sleep, 29(9), 1203–1209. http://doi.org/10.1093/sleep/29.9.1203
El-Ad, B., & Lavie, P. (2005). Effect of sleep apnea on cognition and mood. International Review of Psychiatry, 17(4), 277–282. http://doi.org/10.1080/09540260500104508
Morgenstern, M., Wang, J., Beatty, N., Batemarco, T., Sica, A. L., & Greenberg, H. (2014). Obstructive Sleep Apnea. Endocrinology and Metabolism Clinics of North America, 43(1), 187–204. http://doi.org/10.1016/j.ecl.2013.09.002
Sleep–Related Breathing Disorders in Adults: Recommendations for Syndrome Definition and Measurement Techniques in Clinical Research. (1999). Sleep, 22(5), 667–689. http://doi.org/10.1093/sleep/22.5.667
Ruehland, W. R., Rochford, P. D., O’Donoghue, F. J., Pierce, R. J., Singh, P., & Thornton, A. T. (2009). The New AASM Criteria for Scoring Hypopneas: Impact on the Apnea Hypopnea Index. Sleep, 32(2), 150–157. http://doi.org/10.1093/sleep/32.2.150
Selim, B. J., Koo, B. B., Qin, L., Jeon, S., Won, C., Redeker, N. S., … Yaggi, H. K. (2016). The Association between Nocturnal Cardiac Arrhythmias and Sleep-Disordered Breathing: The DREAM Study. Journal of Clinical Sleep Medicine, 12(06), 829–837. http://doi.org/10.5664/jcsm.5880
Ahmed, M. H. (2010). Obstructive sleep apnea syndrome and fatty liver: Association or causal link? World Journal of Gastroenterology, 16(34), 4243. http://doi.org/10.3748/wjg.v16.i34.4243
Singh, H., Pollock, R., Uhanova, J., Kryger, M., Hawkins, K., & Minuk, G. Y. (2005). Symptoms of Obstructive Sleep Apnea in Patients with Nonalcoholic Fatty Liver Disease. Digestive Diseases and Sciences, 50(12), 2338–2343. http://doi.org/10.1007/s10620-005-3058-y
Lawati, N. M. A., Patel, S. R., & Ayas, N. T. (2009). Epidemiology, Risk Factors, and Consequences of Obstructive Sleep Apnea and Short Sleep Duration. Progress in Cardiovascular Diseases, 51(4), 285–293. http://doi.org/10.1016/j.pcad.2008.08.001
Young, T. (2004). Risk Factors for Obstructive Sleep Apnea in Adults. Jama, 291(16), 2013. http://doi.org/10.1001/jama.291.16.2013
Yaggi, H. K., Concato, J., Kernan, W. N., Lichtman, J. H., Brass, L. M., & Mohsenin, V. (2005). Obstructive Sleep Apnea as a Risk Factor for Stroke and Death. New England Journal of Medicine, 353(19), 2034–2041. http://doi.org/10.1056/nejmoa043104
Redline, S., Budhiraja, R., Kapur, V., Marcus, C. L., Mateika, J. H., Mehra, R., … Quan, A. S. F. (2007). The Scoring of Respiratory Events in Sleep: Reliability and Validity. Journal of Clinical Sleep Medicine, 03(02), 169–200. http://doi.org/10.5664/jcsm.26818
Basheer B, Hegde KS, Bhat SS, Umar D, Baroudi K. Influence of mouth breathing on the dentofacial growth of children: a cephalometric study. J Int Oral Health. 2014;6(6):50-55. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4295456/
Ruhle, K. H., & Nilius, G. (2008). Mouth Breathing in Obstructive Sleep Apnea prior to and during Nasal Continuous Positive Airway Pressure. Respiration, 76(1), 40–45. http://doi.org/10.1159/000111806
Izu, S. C., Itamoto, C. H., Pradella-Hallinan, M., Pizarro, G. U., Tufik, S., Pignatari, S., & Fujita, R. R. (2010). Obstructive sleep apnea syndrome (OSAS) in mouth breathing children. Brazilian Journal of Otorhinolaryngology, 76(5), 552–556. http://doi.org/10.1590/s1808-86942010000500003
Lee, S. H., Choi, J. H., Shin, C., Lee, H. M., Kwon, S. Y., & Lee, S. H. (2007). How Does Open-Mouth Breathing Influence Upper Airway Anatomy? The Laryngoscope, 117(6), 1102–1106. http://doi.org/10.1097/mlg.0b013e318042aef7
Tuomilehto, H. P. I., Seppä, J. M., Partinen, M. M., Peltonen, M., Gylling, H., Tuomilehto, J. O. I., … Uusitupa, M. (2009). Lifestyle Intervention with Weight Reduction. American Journal of Respiratory and Critical Care Medicine, 179(4), 320–327. http://doi.org/10.1164/rccm.200805-669oc
https://www.cdc.gov/nchs/fastats/obesity-overweight.htm
Neill, A. M., Angus, S. M., Sajkov, D., & Mcevoy, R. D. (1997). Effects of sleep posture on upper airway stability in patients with obstructive sleep apnea. American Journal of Respiratory and Critical Care Medicine, 155(1), 199–204. http://doi.org/10.1164/ajrccm.155.1.9001312
Loord, H., & Hultcrantz, E. (2007). Positioner–a method for preventing sleep apnea. Acta Oto-Laryngologica, 127(8), 861–868. http://doi.org/10.1080/00016480601089390
Szollosi, I., Roebuck, T., Thompson, B., & Naughton, M. T. (2006). Lateral Sleeping Position Reduces Severity of Central Sleep Apnea / Cheyne-Stokes Respiration. Sleep, 29(8), 1045–1051. http://doi.org/10.1093/sleep/29.8.1045
Silverberg DS, Iaina A, Oksenberg A. Treating obstructive sleep apnea improves essential hypertension and quality of life. Am Fam Physician. 2002;65(2):229-236. https://pubmed.ncbi.nlm.nih.gov/11820487/
Aurora, R. N., Chowdhuri, S., Ramar, K., Bista, S. R., Casey, K. R., Lamm, C. I., … Tracy, S. L. (2012). The Treatment of Central Sleep Apnea Syndromes in Adults: Practice Parameters with an Evidence-Based Literature Review and Meta-Analyses. Sleep, 35(1), 17–40. http://doi.org/10.5665/sleep.1580
Hsu, A. A. L., & Lo, C. (2003). Continuous positive airway pressure therapy in sleep apnoea. Respirology, 8(4), 447–454. http://doi.org/10.1046/j.1440-1843.2003.00494.x
Patel, S. R., White, D. P., Malhotra, A., Stanchina, M. L., & Ayas, N. T. (2003). Continuous Positive Airway Pressure Therapy for Treating gess in a Diverse Population With Obstructive Sleep Apnea. Archives of Internal Medicine, 163(5), 565. http://doi.org/10.1001/archinte.163.5.565
Sundaram, S., Lim, J., & Lasserson, T. J. (2005). Surgery for obstructive sleep apnoea in adults. Cochrane Database of Systematic Reviews. http://doi.org/10.1002/14651858.cd001004.pub2
Chen, H., & Lowe, A. A. (2012). Updates in oral appliance therapy for snoring and obstructive sleep apnea. Sleep and Breathing, 17(2), 473–486. http://doi.org/10.1007/s11325-012-0712-4
Gaisl, T., Haile, S. R., Thiel, S., Osswald, M., & Kohler, M. (2019). Efficacy of pharmacotherapy for OSA in adults: A systematic review and network meta-analysis. Sleep Medicine Reviews, 46, 74–86. http://doi.org/10.1016/j.smrv.2019.04.009
Ohayon, M., Wickwire, E. M., Hirshkowitz, M., Albert, S. M., Avidan, A., Daly, F. J., … Vitiello, M. V. (2017). National Sleep Foundations sleep quality recommendations: first report. Sleep Health, 3(1), 6–19. http://doi.org/10.1016/j.sleh.2016.11.006
Youngstedt, S. D., Goff, E. E., Reynolds, A. M., Kripke, D. F., Irwin, M. R., Bootzin, R. R., … Jean-Louis, G. (2016). Has adult sleep duration declined over the last 50 years? Sleep Medicine Reviews, 28, 69–85. http://doi.org/10.1016/j.smrv.2015.08.004
Chaput, J.-P., Mcneil, J., Després, J.-P., Bouchard, C., & Tremblay, A. (2013). Seven to Eight Hours of Sleep a Night Is Associated with a Lower Prevalence of the Metabolic Syndrome and Reduced Overall Cardiometabolic Risk in Adults. PLoS ONE, 8(9). http://doi.org/10.1371/journal.pone.0072832
Wild, C. J., Nichols, E. S., Battista, M. E., Stojanoski, B., & Owen, A. M. (2018). Dissociable effects of self-reported daily sleep duration on high-level cognitive abilities. Sleep, 41(12). http://doi.org/10.1093/sleep/zsy182
Hirshkowitz, M., Whiton, K., Albert, S. M., Alessi, C., Bruni, O., Doncarlos, L., … Hillard, P. J. A. (2015). National Sleep Foundation’s sleep time duration recommendations: methodology and results summary. Sleep Health, 1(1), 40–43. http://doi.org/10.1016/j.sleh.2014.12.010
Cappuccio, F. P., Delia, L., Strazzullo, P., & Miller, M. A. (2010). Sleep Duration and All-Cause Mortality: A Systematic Review and Meta-Analysis of Prospective Studies. Sleep, 33(5), 585–592. http://doi.org/10.1093/sleep/33.5.585
Gottlieb, D. J., Punjabi, N. M., Newman, A. B., Resnick, H. E., Redline, S., Baldwin, C. M., & Nieto, F. J. (2005). Association of Sleep Time With Diabetes Mellitus and Impaired Glucose Tolerance. Archives of Internal Medicine, 165(8), 863. http://doi.org/10.1001/archinte.165.8.863
Short, M. A., Agostini, A., Lushington, K., & Dorrian, J. (2015). A systematic review of the sleep, sleepiness, and performance implications of limited wake shift work schedules. Scandinavian Journal of Work, Environment & Health, 41(5), 425–440. http://doi.org/10.5271/sjweh.3509
Cappuccio, F. P., Taggart, F. M., Kandala, N.-B., Currie, A., Peile, E., Stranges, S., & Miller, M. A. (2008). Meta-Analysis of Short Sleep Duration and Obesity in Children and Adults. Sleep, 31(5), 619–626. http://doi.org/10.1093/sleep/31.5.619
Mong, J. A., & Cusmano, D. M. (2016). Sex differences in sleep: impact of biological sex and sex steroids. Philosophical Transactions of the Royal Society B: Biological Sciences, 371(1688), 20150110. http://doi.org/10.1098/rstb.2015.0110
Krishnan, V., & Collop, N. A. (2006). Gender differences in sleep disorders. Current Opinion in Pulmonary Medicine, 12(6), 383–389. http://doi.org/10.1097/01.mcp.0000245705.69440.6a
Mehta, N., Shafi, F., & Bhat, A. (2015). Unique Aspects of Sleep in Women. Missouri medicine, 112(6), 430–434. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6168103/
Moline, M. L., Broch, L., & Zak, R. (2004). Sleep in women across the life cycle from adulthood through menopause. Medical Clinics of North America, 88(3), 705–736. http://doi.org/10.1016/j.mcna.2004.01.009
He, Y., Jones, C. R., Fujiki, N., Xu, Y., Guo, B., Holder, J. L., … Fu, Y.-H. (2009). The Transcriptional Repressor DEC2 Regulates Sleep Length in Mammals. Science, 325(5942), 866–870. http://doi.org/10.1126/science.1174443
Theorell-Haglöw, J., Berglund, L., Berne, C., & Lindberg, E. (2014). Both habitual short sleepers and long sleepers are at greater risk of obesity: a population-based 10-year follow-up in women. Sleep Medicine, 15(10), 1204–1211. http://doi.org/10.1016/j.sleep.2014.02.014
Mezick, E. J., Wing, R. R., & Mccaffery, J. M. (2014). Associations of self-reported and actigraphy-assessed sleep characteristics with body mass index and waist circumference in adults: moderation by gender. Sleep Medicine, 15(1), 64–70. http://doi.org/10.1016/j.sleep.2013.08.784
Kim, S. J. (2011). Relationship Between Weekend Catch-up Sleep and Poor Performance on Attention Tasks in Korean Adolescents. Archives of Pediatrics & Adolescent Medicine, 165(9), 806. http://doi.org/10.1001/archpediatrics.2011.128
Kim, C.-W., Choi, M.-K., Im, H.-J., Kim, O.-H., Lee, H.-J., Song, J., … Park, K.-H. (2012). Weekend catch-up sleep is associated with decreased risk of being overweight among fifth-grade students with short sleep duration. Journal of Sleep Research, 21(5), 546–551. http://doi.org/10.1111/j.1365-2869.2012.01013.x
Sun, W., Ling, J., Zhu, X., Lee, T. M.-C., & Li, S. X. (2019). Associations of weekday-to-weekend sleep differences with academic performance and health-related outcomes in school-age children and youths. Sleep Medicine Reviews, 46, 27–53. http://doi.org/10.1016/j.smrv.2019.04.003
Kang, S.-G., Lee, Y. J., Kim, S. J., Lim, W., Lee, H.-J., Park, Y.-M., … Hong, J. P. (2014). Weekend catch-up sleep is independently associated with suicide attempts and self-injury in Korean adolescents. Comprehensive Psychiatry, 55(2), 319–325. http://doi.org/10.1016/j.comppsych.2013.08.023
Zhao, M., Tuo, H., Wang, S., & Zhao, L. (2020). The Effects of Dietary Nutrition on Sleep and Sleep Disorders. Mediators of Inflammation, 2020, 1–7. http://doi.org/10.1155/2020/3142874
Doherty, Madigan, Warrington, & Ellis. (2019). Sleep and Nutrition Interactions: Implications for Athletes. Nutrients, 11(4), 822. http://doi.org/10.3390/nu11040822
Sutanto CN, Wang MX, Tan D, Kim JE. Association of Sleep Quality and Macronutrient Distribution: A Systematic Review and Meta-Regression. Nutrients. 2020 Jan 2;12(1):126. doi: 10.3390/nu12010126. PMID: 31906452; PMCID: PMC7019667. https://pubmed.ncbi.nlm.nih.gov/31906452/
Peuhkuri, K., Sihvola, N., & Korpela, R. (2012). Diet promotes sleep duration and quality. Nutrition Research, 32(5), 309–319. http://doi.org/10.1016/j.nutres.2012.03.009
Afaghi, A., Oconnor, H., & Chow, C. M. (2007). High-glycemic-index carbohydrate meals shorten sleep onset. The American Journal of Clinical Nutrition, 85(2), 426–430. http://doi.org/10.1093/ajcn/85.2.426
Golem, D. L., Martin-Biggers, J. T., Koenings, M. M., Davis, K. F., & Byrd-Bredbenner, C. (2014). An Integrative Review of Sleep for Nutrition Professionals. Advances in Nutrition, 5(6), 742–759. http://doi.org/10.3945/an.114.006809
Grandner, M. A., Jackson, N., Gerstner, J. R., & Knutson, K. L. (2013). Sleep symptoms associated with intake of specific dietary nutrients. Journal of Sleep Research, 23(1), 22–34. http://doi.org/10.1111/jsr.12084
Porter, J., & Horne, J. (1981). Bed-time food supplements and sleep: Effects of different carbohydrate levels. Electroencephalography and Clinical Neurophysiology, 51(4), 426–433. http://doi.org/10.1016/0013-4694(81)90106-1
Halson, S. L. (2014). Sleep in Elite Athletes and Nutritional Interventions to Enhance Sleep. Sports Medicine, 44(S1), 13–23. http://doi.org/10.1007/s40279-014-0147-0
Rondanelli, M., Opizzi, A., Monteferrario, F., Antoniello, N., Manni, R., & Klersy, C. (2011). The Effect of Melatonin, Magnesium, and Zinc on Primary Insomnia in Long-Term Care Facility Residents in Italy: A Double-Blind, Placebo-Controlled Clinical Trial. Journal of the American Geriatrics Society, 59(1), 82–90. http://doi.org/10.1111/j.1532-5415.2010.03232.x
Tahara, Y., & Shibata, S. (2014). Chrono-biology, Chrono-pharmacology, and Chrono-nutrition. Journal of Pharmacological Sciences, 124(3), 320–335. http://doi.org/10.1254/jphs.13r06cr
Landolt, H.-P., Werth, E., Borbély, A. A., & Dijk, D.-J. (1995). Caffeine intake (200 mg) in the morning affects human sleep and EEG power spectra at night. Brain Research, 675(1-2), 67–74. http://doi.org/10.1016/0006-8993(95)00040-w
Gottesmann, C. (2002). GABA mechanisms and sleep. Neuroscience, 111(2), 231–239. http://doi.org/10.1016/s0306-4522(02)00034-9
Campbell, S. S., Dawson, D., & Anderson, M. W. (1993). Alleviation of Sleep Maintenance Insomnia with Timed Exposure to Bright Light. Journal of the American Geriatrics Society, 41(8), 829–836. http://doi.org/10.1111/j.1532-5415.1993.tb06179.x
Zhao, J., Tian, Y., Nie, J., Xu, J., & Liu, D. (2012). Red Light and the Sleep Quality and Endurance Performance of Chinese Female Basketball Players. Journal of Athletic Training, 47(6), 673–678. http://doi.org/10.4085/1062-6050-47.6.08
Smolensky, M. H., Sackett-Lundeen, L. L., & Portaluppi, F. (2015). Nocturnal light pollution and underexposure to daytime sunlight: Complementary mechanisms of circadian disruption and related diseases. Chronobiology International, 32(8), 1029–1048. http://doi.org/10.3109/07420528.2015.1072002
Düzgün, G., & Akyol, A. D. (2017). Effect of Natural Sunlight on Sleep Problems and Sleep Quality of the Elderly Staying in the Nursing Home. Holistic Nursing Practice, 31(5), 295–302. http://doi.org/10.1097/hnp.0000000000000206
Valham, F., Sahlin, C., Stenlund, H., & Franklin, K. A. (2012). Ambient Temperature and Obstructive Sleep Apnea: Effects on Sleep, Sleep Apnea, and Morning Alertness. Sleep, 35(4), 513–517. http://doi.org/10.5665/sleep.1736
Okamoto-Mizuno, K., Tsuzuki, K., & Mizuno, K. (2004). Effects of mild heat exposure on sleep stages and body temperature in older men. International Journal of Biometeorology, 49(1). http://doi.org/10.1007/s00484-004-0209-3
St-Onge, M.-P., & Shechter, A. (2014). Sleep disturbances, body fat distribution, food intake and/or energy expenditure: pathophysiological aspects. Hormone Molecular Biology and Clinical Investigation, 17(1). http://doi.org/10.1515/hmbci-2013-0066
Chaput, J.-P., Després, J.-P., Bouchard, C., & Tremblay, A. (2008). The Association Between Sleep Duration and Weight Gain in Adults: A 6-Year Prospective Study from the Quebec Family Study. Sleep, 31(4), 517–523. http://doi.org/10.1093/sleep/31.4.517
Dekker, S. A., Noordam, R., Biermasz, N. R., Roos, A., Lamb, H. J., Rosendaal, F. R., … Mutsert, R. (2018). Habitual Sleep Measures are Associated with Overall Body Fat, and not Specifically with Visceral Fat, in Men and Women. Obesity, 26(10), 1651–1658. http://doi.org/10.1002/oby.22289
Tunnicliffe, J. M., Erdman, K. A., Reimer, R. A., Lun, V., & Shearer, J. (2008). Consumption of dietary caffeine and coffee in physically active populations: physiological interactions. Applied Physiology, Nutrition, and Metabolism, 33(6), 1301–1310. http://doi.org/10.1139/h08-124
Mahoney, C. R., Giles, G. E., Marriott, B. P., Judelson, D. A., Glickman, E. L., Geiselman, P. J., & Lieberman, H. R. (2019). Intake of caffeine from all sources and reasons for use by college students. Clinical Nutrition, 38(2), 668–675. http://doi.org/10.1016/j.clnu.2018.04.004
Binks, H., Vincent, G. E., Gupta, C., Irwin, C., & Khalesi, S. (2020). Effects of Diet on Sleep: A Narrative Review. Nutrients, 12(4), 936. http://doi.org/10.3390/nu12040936
Rao, T. P., Ozeki, M., & Juneja, L. R. (2015). In Search of a Safe Natural Sleep Aid. Journal of the American College of Nutrition, 34(5), 436–447. http://doi.org/10.1080/07315724.2014.926153
Abbasi B, Kimiagar M, Sadeghniiat K, Shirazi MM, Hedayati M, Rashidkhani B. The effect of magnesium supplementation on primary insomnia in elderly: A double-blind placebo-controlled clinical trial. J Res Med Sci. 2012 Dec;17(12):1161-9. https://pubmed.ncbi.nlm.nih.gov/23853635/
Aspy, D. J., Madden, N. A., & Delfabbro, P. (2018). Effects of Vitamin B6 (Pyridoxine) and a B Complex Preparation on Dreaming and Sleep. Perceptual and Motor Skills, 003151251877032. http://doi.org/10.1177/0031512518770326
Parazzini F. Resveratrol, tryptophanum, glycine and vitamin E: a nutraceutical approach to sleep disturbance and irritability in peri- and post-menopause. Minerva Ginecol. 2015;67(1):1-5. https://pubmed.ncbi.nlm.nih.gov/25660429/
Siegel JM. The neurotransmitters of sleep. J Clin Psychiatry. 2004;65 Suppl 16:4-7. https://pubmed.ncbi.nlm.nih.gov/15575797/
Djeridane, Y., Touitou, Y. Chronic diazepam administration differentially affects melatonin synthesis in rat pineal and Harderian glands. Psychopharmacology154, 403–407 (2001). https://doi.org/10.1007/s002130000631
Betti L, Palego L, Demontis GC, Miraglia F, Giannaccini G. Hydroxyindole-O-methyltransferase (HIOMT) activity in the retina of melatonin-proficient mice. Heliyon. 2019;5(9):e02417. Published 2019 Sep 14. doi:10.1016/j.heliyon.2019.e02417
Haduch, A., Bromek, E., Wójcikowski, J., Gołembiowska, K., Daniel, W.. Melatonin Supports Serotonin Formation by Brain CYP2D. Drug Metabolism and DispositionMarch 1, 2016, 44 (3) 445-452; DOI: https://doi.org/10.1124/dmd.115.067413
Morton, D. J. (1987). Mechanism of Inhibition of Bovine Pineal Gland Hydroxyindole-O-Methyltransferase (EC 2.1.1.4) by Divalent Cations. Journal of Pineal Research, 4(3), 295–303. http://doi.org/10.1111/j.1600-079x.1987.tb00867.x
Markova-Car, E. P., Jurišić, D., Ilić, N., & Pavelić, S. K. (2014). Running for time: circadian rhythms and melanoma. Tumor Biology, 35(9), 8359–8368. http://doi.org/10.1007/s13277-014-1904-2
Slominski AT, Zmijewski MA, Skobowiat C, Zbytek B, Slominski RM, Steketee JD. Sensing the environment: regulation of local and global homeostasis by the skin’s neuroendocrine system. Adv Anat Embryol Cell Biol. 2012;212:v-115. doi:10.1007/978-3-642-19683-6_1 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3422784/
Chalupsky, K., Kračun, D., Kanchev, I., Bertram, K., & Görlach, A. (2015). Folic Acid Promotes Recycling of Tetrahydrobiopterin and Protects Against Hypoxia-Induced Pulmonary Hypertension by Recoupling Endothelial Nitric Oxide Synthase. Antioxidants & Redox Signaling, 23(14), 1076–1091. http://doi.org/10.1089/ars.2015.6329
Dianzani, I., Sanctis, L. D., Smooker, P. M., Gough, T. J., Alliaudi, C., Brusco, A., … Cotton, R. G. H. (1998). Dihydropteridine reductase deficiency: Physical structure of the QDPR gene, identification of two new mutations and genotype–phenotype correlations. Human Mutation, 12(4), 267–273. http://doi.org/10.1002/(sici)1098-1004(1998)12:4<267::aid-humu8>3.0.co;2-c
Nichol, C. A., Lee, C. L., Edelstein, M. P., Chao, J. Y., & Duch, D. S. (1983). Biosynthesis of tetrahydrobiopterin by de novo and salvage pathways in adrenal medulla extracts, mammalian cell cultures, and rat brain in vivo. Proceedings of the National Academy of Sciences, 80(6), 1546–1550. http://doi.org/10.1073/pnas.80.6.1546
Titus, F., Dávalos, A., Alom, J., & Codina, A. (1986). 5-Hydroxytryptophan versus Methysergide in the Prophylaxis of Migraine. European Neurology, 25(5), 327–329. http://doi.org/10.1159/000116030
Birdsall TC. 5-Hydroxytryptophan: a clinically-effective serotonin precursor. Altern Med Rev. 1998;3(4):271-280. https://pubmed.ncbi.nlm.nih.gov/9727088/
Volpi-Abadie J, Kaye AM, Kaye AD. Serotonin syndrome. Ochsner J. 2013;13(4):533-540. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3865832/
Valadas, J. S., Esposito, G., Vandekerkhove, D., Miskiewicz, K., Deaulmerie, L., Raitano, S., … Verstreken, P. (2018). ER Lipid Defects in Neuropeptidergic Neurons Impair Sleep Patterns in Parkinson’s Disease. Neuron, 98(6). http://doi.org/10.1016/j.neuron.2018.05.022
Chung SY, Moriyama T, Uezu E, et al. Administration of phosphatidylcholine increases brain acetylcholine concentration and improves memory in mice with dementia. J Nutr. 1995;125(6):1484-1489. doi:10.1093/jn/125.6.1484 https://pubmed.ncbi.nlm.nih.gov/7782901/
Montgomery, P., Burton, J. R., Sewell, R. P., Spreckelsen, T. F., & Richardson, A. J. (2014). Fatty acids and sleep in UK children: subjective and pilot objective sleep results from the DOLAB study – a randomized controlled trial. Journal of Sleep Research, 23(4), 364–388. http://doi.org/10.1111/jsr.12135
Alzoubi, K. H., Mayyas, F., & Zamzam, H. I. A. (2019). Omega-3 fatty acids protects against chronic sleep-deprivation induced memory impairment. Life Sciences, 227, 1–7. http://doi.org/10.1016/j.lfs.2019.04.028
Nasehi, M., Mosavi-Nezhad, S.-M., Khakpai, F., & Zarrindast, M.-R. (2018). The role of omega-3 on modulation of cognitive deficiency induced by REM sleep deprivation in rats. Behavioural Brain Research, 351, 152–160. http://doi.org/10.1016/j.bbr.2018.06.002
Jahangard, L., Sadeghi, A., Ahmadpanah, M., Holsboer-Trachsler, E., Bahmani, D. S., Haghighi, M., & Brand, S. (2018). Influence of adjuvant omega-3-polyunsaturated fatty acids on depression, sleep, and emotion regulation among outpatients with major depressive disorders – Results from a double-blind, randomized and placebo-controlled clinical trial. Journal of Psychiatric Research, 107, 48–56. http://doi.org/10.1016/j.jpsychires.2018.09.016
Scorza, F. A., Cavalheiro, E. A., Scorza, C. A., Galduróz, J. C. F., Tufik, S., & Andersen, M. L. (2013). Sleep Apnea and Inflammation – Getting a Good Night’s Sleep with Omega-3 Supplementation. Frontiers in Neurology, 4. http://doi.org/10.3389/fneur.2013.00193
Hansen, A. L., Dahl, L., Olson, G., Thornton, D., Graff, I. E., Frøyland, L., … Pallesen, S. (2014). Fish Consumption, Sleep, Daily Functioning, and Heart Rate Variability. Journal of Clinical Sleep Medicine, 10(05), 567–575. http://doi.org/10.5664/jcsm.3714
Xie, L., Kang, H., Xu, Q., Chen, M. J., Liao, Y., Thiyagarajan, M., … Nedergaard, M. (2013). Sleep Drives Metabolite Clearance from the Adult Brain. Science, 342(6156), 373–377. http://doi.org/10.1126/science.1241224
Varshavsky, A. (2012). Augmented generation of protein fragments during wakefulness as the molecular cause of sleep: a hypothesis. Protein Science, 21(11), 1634–1661. http://doi.org/10.1002/pro.2148
Mackiewicz, M., Shockley, K. R., Romer, M. A., Galante, R. J., Zimmerman, J. E., Naidoo, N., … Pack, A. I. (2007). Macromolecule biosynthesis: a key function of sleep. Physiological Genomics, 31(3), 441–457. http://doi.org/10.1152/physiolgenomics.00275.2006
Scharf, M. T., Naidoo, N., Zimmerman, J. E., & Pack, A. I. (2008). The energy hypothesis of sleep revisited. Progress in Neurobiology, 86(3), 264–280. http://doi.org/10.1016/j.pneurobio.2008.08.003
Horne, J. (2009). REM sleep, energy balance and ‘optimal foraging.’ Neuroscience & Biobehavioral Reviews, 33(3), 466–474. http://doi.org/10.1016/j.neubiorev.2008.12.002
Berger, R. J., & Phillips, N. H. (1995). Energy conservation and sleep. Behavioural Brain Research, 69(1-2), 65–73. http://doi.org/10.1016/0166-4328(95)00002-b
Benington, J. H., & Heller, H. C. (1995). Restoration of brain energy metabolism as the function of sleep. Progress in Neurobiology, 45(4), 347–360. http://doi.org/10.1016/0301-0082(94)00057-o
Abel, T., Havekes, R., Saletin, J. M., & Walker, M. P. (2013). Sleep, Plasticity and Memory from Molecules to Whole-Brain Networks. Current Biology, 23(17). http://doi.org/10.1016/j.cub.2013.07.025
Rasch, B., & Born, J. (2013). About Sleeps Role in Memory. Physiological Reviews, 93(2), 681–766. http://doi.org/10.1152/physrev.00032.2012
Cirelli, C., & Tononi, G. (2008). Is Sleep Essential? PLoS Biology, 6(8). http://doi.org/10.1371/journal.pbio.0060216
Siegel, J. M. (2005). Clues to the functions of mammalian sleep. Nature, 437(7063), 1264–1271. http://doi.org/10.1038/nature04285
Campbell, S. S., & Tobler, I. (1984). Animal sleep: A review of sleep duration across phylogeny. Neuroscience & Biobehavioral Reviews, 8(3), 269–300. http://doi.org/10.1016/0149-7634(84)90054-x
Tobler, I. (1995). Is sleep fundamentally different between mammalian species? Behavioural Brain Research, 69(1-2), 35–41. http://doi.org/10.1016/0166-4328(95)00025-o
Tononi, G., & Cirelli, C. (2006). Sleep function and synaptic homeostasis. Sleep Medicine Reviews, 10(1), 49–62. http://doi.org/10.1016/j.smrv.2005.05.002
Dongen, H. P. A. V., Vitellaro, K. M., & Dinges, D. F. (2005). Individual Differences in Adult Human Sleep and Wakefulness: Leitmotif for a Research Agenda. Sleep, 28(4), 479–498. http://doi.org/10.1093/sleep/28.4.479
Vyazovskiy, V. V., & Delogu, A. (2014). NREM and REM Sleep. The Neuroscientist, 20(3), 203–219. http://doi.org/10.1177/1073858413518152
Mignot, E. (2008). Why We Sleep: The Temporal Organization of Recovery. PLoS Biology, 6(4). http://doi.org/10.1371/journal.pbio.0060106
Siegel, J. M. (2009). Sleep viewed as a state of adaptive inactivity. Nature Reviews Neuroscience, 10(10), 747–753. http://doi.org/10.1038/nrn2697
Horne, J. (2000). REM sleep — by default? Neuroscience & Biobehavioral Reviews, 24(8), 777–797. http://doi.org/10.1016/s0149-7634(00)00037-3
Baran, B., Pace-Schott, E. F., Ericson, C., & Spencer, R. M. C. (2012). Processing of Emotional Reactivity and Emotional Memory over Sleep. Journal of Neuroscience, 32(3), 1035–1042. http://doi.org/10.1523/jneurosci.2532-11.2012
Tononi, G., & Cirelli, C. (2014). Sleep and the Price of Plasticity: From Synaptic and Cellular Homeostasis to Memory Consolidation and Integration. Neuron, 81(1), 12–34. http://doi.org/10.1016/j.neuron.2013.12.025
Li, J., Vitiello, M. V., & Gooneratne, N. S. (2018). Sleep in Normal Aging. Sleep Medicine Clinics, 13(1), 1–11. http://doi.org/10.1016/j.jsmc.2017.09.001
Murillo-Rodriguez, E., Arias-Carrion, O., Zavala-Garcia, A., Sarro-Ramirez, A., & Huitron-Resendiz, S. (2012). Basic Sleep Mechanisms: An Integrative Review. Central Nervous System Agents in Medicinal Chemistry, 12(1), 38–54. http://doi.org/10.2174/187152412800229107
Weber, F. D. (2018). Sleep: Eye-Opener Highlights Sleep’s Organization. Current Biology, 28(5). http://doi.org/10.1016/j.cub.2018.01.054
Yetton, B. D., Mcdevitt, E. A., Cellini, N., Shelton, C., & Mednick, S. C. (2018). Quantifying sleep architecture dynamics and individual differences using big data and Bayesian networks. Plos One, 13(4). http://doi.org/10.1371/journal.pone.0194604
Colrain, I. M., Nicholas, C. L., & Baker, F. C. (2014). Alcohol and the sleeping brain. Handbook of Clinical Neurology Alcohol and the Nervous System, 415–431. http://doi.org/10.1016/b978-0-444-62619-6.00024-0
Zisapel, N. (2018). New perspectives on the role of melatonin in human sleep, circadian rhythms and their regulation. British Journal of Pharmacology, 175(16), 3190–3199. http://doi.org/10.1111/bph.14116
Tosini, G., Baba, K., Hwang, C. K., & Iuvone, P. M. (2012). Melatonin: An underappreciated player in retinal physiology and pathophysiology. Experimental Eye Research, 103, 82–89. http://doi.org/10.1016/j.exer.2012.08.009
Blasiak, J., Reiter, R. J., & Kaarniranta, K. (2016). Melatonin in Retinal Physiology and Pathology: The Case of Age-Related Macular Degeneration. Oxidative Medicine and Cellular Longevity, 2016, 1–12. http://doi.org/10.1155/2016/6819736
Bellingham, J., Chaurasia, S. S., Melyan, Z., Liu, C., Cameron, M. A., Tarttelin, E. E., … Lucas, R. J. (2006). Evolution of Melanopsin Photoreceptors: Discovery and Characterization of a New Melanopsin in Nonmammalian Vertebrates. PLoS Biology, 4(8). http://doi.org/10.1371/journal.pbio.0040254
Zaidi, F. H., Hull, J. T., Peirson, S. N., Wulff, K., Aeschbach, D., Gooley, J. J., … Lockley, S. W. (2007). Short-Wavelength Light Sensitivity of Circadian, Pupillary, and Visual Awareness in Humans Lacking an Outer Retina. Current Biology, 17(24), 2122–2128. http://doi.org/10.1016/j.cub.2007.11.034
Legates, T. A., Altimus, C. M., Wang, H., Lee, H.-K., Yang, S., Zhao, H., … Hattar, S. (2012). Aberrant light directly impairs mood and learning through melanopsin-expressing neurons. Nature, 491(7425), 594–598. http://doi.org/10.1038/nature11673
Sikka, G., Hussmann, G. P., Pandey, D., Cao, S., Hori, D., Park, J. T., … Berkowitz, D. E. (2014). Melanopsin mediates light-dependent relaxation in blood vessels. Proceedings of the National Academy of Sciences, 111(50), 17977–17982. http://doi.org/10.1073/pnas.1420258111
Buhr, E. D., Yoo, S.-H., & Takahashi, J. S. (2010). Temperature as a Universal Resetting Cue for Mammalian Circadian Oscillators. Science, 330(6002), 379–385. http://doi.org/10.1126/science.1195262
Robbins, R., Grandner, M. A., Buxton, O. M., Hale, L., Buysse, D. J., Knutson, K. L., … Jean-Louis, G. (2019). Sleep myths: an expert-led study to identify false beliefs about sleep that impinge upon population sleep health practices. Sleep Health, 5(4), 409–417. http://doi.org/10.1016/j.sleh.2019.02.002
Damiola, F. (2000). Restricted feeding uncouples circadian oscillators in peripheral tissues from the central pacemaker in the suprachiasmatic nucleus. Genes & Development, 14(23), 2950–2961. http://doi.org/10.1101/gad.183500
Abel, T., Havekes, R., Saletin, J. M., & Walker, M. P. (2013). Sleep, Plasticity and Memory from Molecules to Whole-Brain Networks. Current Biology, 23(17). http://doi.org/10.1016/j.cub.2013.07.025
Muzet, A., Ehrhart, J., Candas, V., Libert, J. P., & Vogt, J. J. (1983). Rem Sleep and Ambient Temperature in Man. International Journal of Neuroscience, 18(1-2), 117–125. http://doi.org/10.3109/00207458308985885
Saini, C., Morf, J., Stratmann, M., Gos, P., & Schibler, U. (2012). Simulated body temperature rhythms reveal the phase-shifting behavior and plasticity of mammalian circadian oscillators. Genes & Development, 26(6), 567–580. http://doi.org/10.1101/gad.183251.111
Franco P, Szliwowski H, Dramaix M, Kahn A. Influence of ambient temperature on sleep characteristics and autonomic nervous control in healthy infants. Sleep. 2000 May 1;23(3):401-7. https://pubmed.ncbi.nlm.nih.gov/10811384/
Libert JP, Candas V, Muzet A, Ehrhart J. Thermoregulatory adjustments to thermal transients during slow wave sleep and REM sleep in man. J Physiol (Paris). 1982;78(3):251-7 https://pubmed.ncbi.nlm.nih.gov/7166740/
Palca, J. W., Walker, J. M., & Berger, R. J. (1986). Thermoregulation, metabolism, and stages of sleep in cold-exposed men. Journal of Applied Physiology, 61(3), 940–947. http://doi.org/10.1152/jappl.1986.61.3.940
Lack. (2009). Chronotype differences in circadian rhythms of temperature, melatonin, and sleepiness as measured in a modified constant routine protocol. Nature and Science of Sleep, 1. http://doi.org/10.2147/nss.s6234
Samson, D. R., Crittenden, A. N., Mabulla, I. A., Mabulla, A. Z. P., & Nunn, C. L. (2017). Chronotype variation drives night-time sentinel-like behaviour in hunter–gatherers. Proceedings of the Royal Society B: Biological Sciences, 284(1858), 20170967. http://doi.org/10.1098/rspb.2017.0967
Walker, R. J., Kribs, Z. D., Christopher, A. N., Shewach, O. R., & Wieth, M. B. (2014). Age, the Big Five, and time-of-day preference: A mediational model. Personality and Individual Differences, 56, 170–174. http://doi.org/10.1016/j.paid.2013.09.003
Bjorness, T., & Greene, R. (2009). Adenosine and Sleep. Current Neuropharmacology, 7(3), 238–245. http://doi.org/10.2174/157015909789152182
Dworak, M., Diel, P., Voss, S., Hollmann, W., & Strüder, H. (2007). Intense exercise increases adenosine concentrations in rat brain: Implications for a homeostatic sleep drive. Neuroscience, 150(4), 789–795. http://doi.org/10.1016/j.neuroscience.2007.09.062
Rainnie, D., Grunze, H., Mccarley, R., & Greene, R. (1994). Adenosine inhibition of mesopontine cholinergic neurons: implications for EEG arousal. Science, 263(5147), 689–692. http://doi.org/10.1126/science.8303279
Daly, J. W., Shi, D., Nikodijevic, O., & Jacobson, K. A. (1994). The role of adenosine receptors in the central action of caffeine. Pharmacopsychoecologia, 7(2), 201–213. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4373791/